
Maternal-Fetal Medicine — MCQs

On this page
In which of the following clinical scenarios is Anti-D prophylaxis not recommended?
What is the most common congenital heart disease during pregnancy?
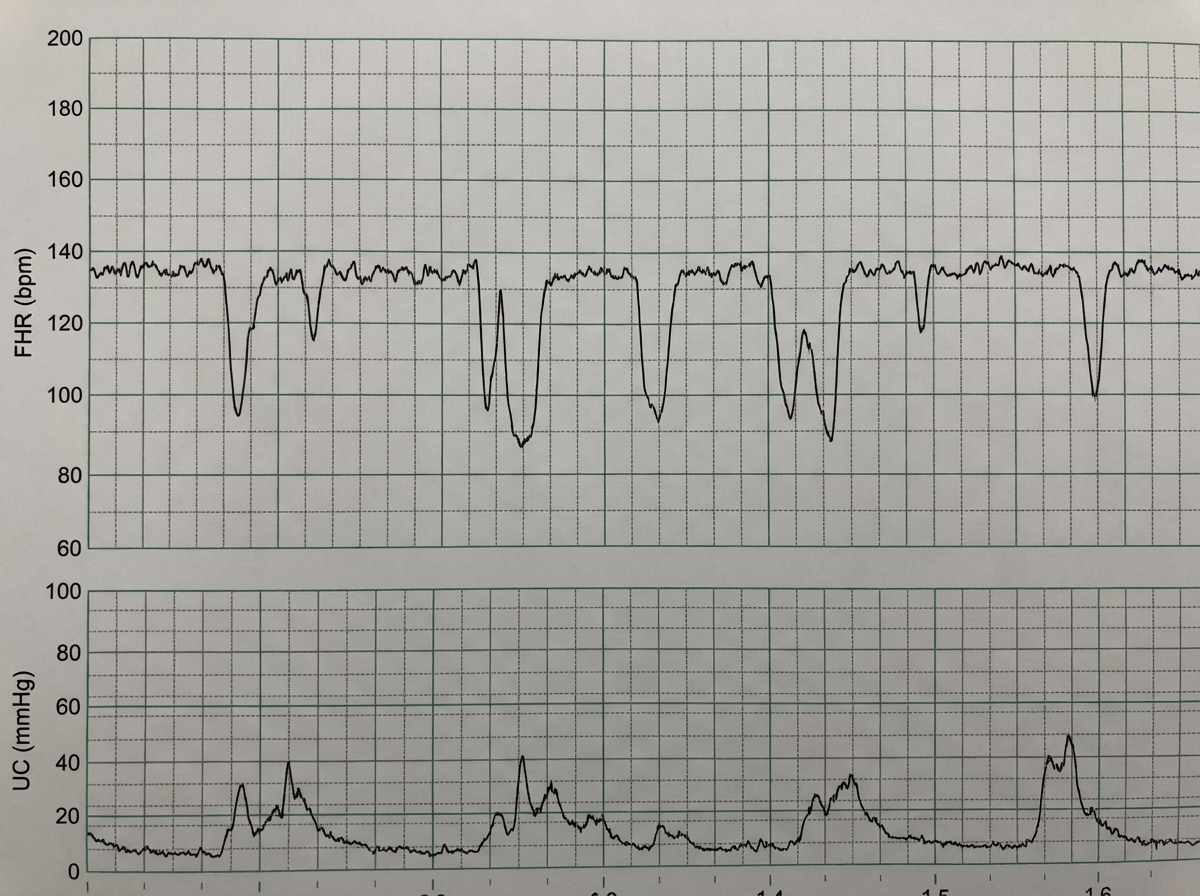
A 28-year-old woman, gravida 4 para 3 living 2 abortion 1, at 35 weeks of gestation with a monochorionic monoamniotic twin pregnancy was admitted for safe confinement. Three days following admission, the Non-stress test (NST) showed the following finding: What is the finding shown in the NST?
Which of the following is NOT associated with hydramnios?
The "lambda sign" or "twin peak sign" is seen in which type of twin pregnancy?
Cord blood gas and pH analysis is done in the following circumstances, except?
With regards to acute pyelonephritis in pregnancy, all of the following are true except:
A woman presents with right-sided lower abdominal pain and mild vaginal bleeding at 6 weeks of gestation. Her general condition is satisfactory, and a urine hCG test is positive. Transvaginal ultrasound reveals an adnexal mass measuring 30 mm in diameter without cardiac activity, and no intrauterine pregnancy is seen. What is the most appropriate management?
In gestational hypertension, hypertension should resolve by how many weeks in the postpartum period?
A G2P1 patient on warfarin presents at 38 weeks in labor. What is the next step in management?
Practice by Chapter
Fetal Assessment Techniques
Practice Questions
Hypertensive Disorders in Pregnancy
Practice Questions
Intrauterine Growth Restriction
Practice Questions
Multiple Gestation
Practice Questions
Rh Isoimmunization and Other Blood Group Incompatibilities
Practice Questions
Intrauterine Fetal Therapy
Practice Questions
Prenatal Diagnosis and Genetic Counseling
Practice Questions
Placental Abnormalities
Practice Questions
Preterm Labor and Delivery
Practice Questions
Management of Medical Disorders in Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app