
Maternal-Fetal Medicine — MCQs

On this page
Which of the following statements regarding cholestasis in pregnancy is false?
Which of the following tests on amniotic fluid is most useful in distinguishing between open neural tube defects and ventral wall defects in a fetus?
In a macerated baby, the ideal sample for genetic analysis is obtained from:
Which of the following procedures is not performed in a case of complete hydatidiform mole (CHM)?
Sonography of a term multigravida shows an amniotic fluid index of 3 cm. The fetus may have which condition?
Vasa previa in a term gestation is managed by __________.
Which of the following is NOT a characteristic of the recipient twin in a monochorionic twin gestation affected by twin-twin transfusion syndrome?
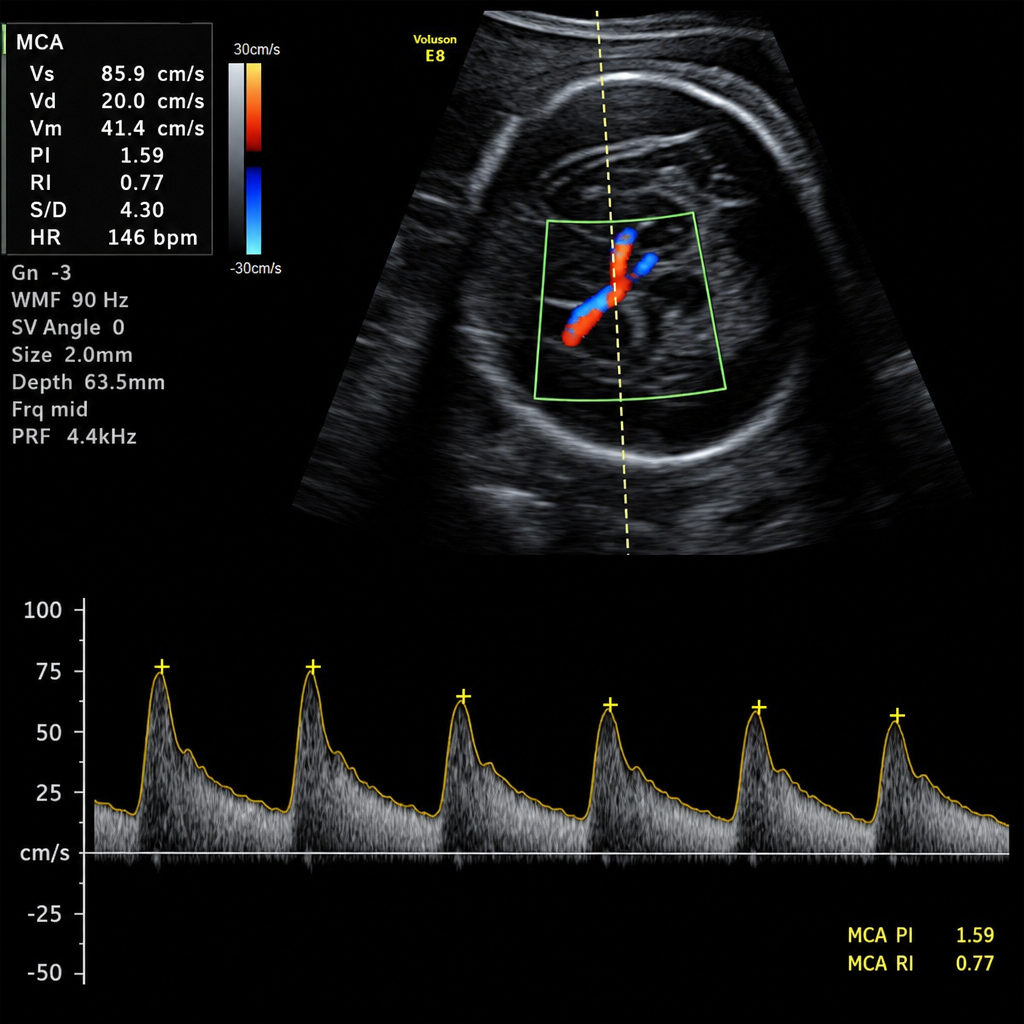
A 28-week pregnant female presents with fetal distress on examination, and the MCA Doppler study is as follows. What should be the next step in management?
A 30-year-old primigravida at 36 weeks of pregnancy presents with a blood pressure of 160/110 mmHg, 3+ urinary albumin, and a platelet count of 80,000/mm3. What is the most appropriate management option?
A female with 6 weeks of amenorrhea presents with an ovarian cyst that requires surgical intervention. The optimal timing for surgery is:
Practice by Chapter
Fetal Assessment Techniques
Practice Questions
Hypertensive Disorders in Pregnancy
Practice Questions
Intrauterine Growth Restriction
Practice Questions
Multiple Gestation
Practice Questions
Rh Isoimmunization and Other Blood Group Incompatibilities
Practice Questions
Intrauterine Fetal Therapy
Practice Questions
Prenatal Diagnosis and Genetic Counseling
Practice Questions
Placental Abnormalities
Practice Questions
Preterm Labor and Delivery
Practice Questions
Management of Medical Disorders in Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app