
Maternal-Fetal Medicine — MCQs

On this page
A female patient presents to you with six weeks of amenorrhea, associated with abdominal pain and vaginal bleeding with normal blood pressure. Investigations revealed beta-hCG to be 1400 mIU/mL. An ultrasound scan was done which showed a trilaminar endometrium with normal adnexa. What is the next best step in the management of this patient?
In a case of DCDA twins at 38 weeks, with the first twin in breech presentation, and the mother having a blood pressure of 140/96 and 1+ proteinuria, what is the preferred management?
A primigravida at 22 weeks of gestation presents with profuse vaginal bleeding. Her blood pressure and glucose levels are normal. At which of the following sites can placental implantation lead to this condition?
A 22-year-old primigravida visits ANC OPD with 20 weeks POG. On examination uterine height reveals a 16-week size. USG shows reduced liquor. What will be the diagnosis?
Which of the following statement is correct about acute fatty liver of pregnancy?
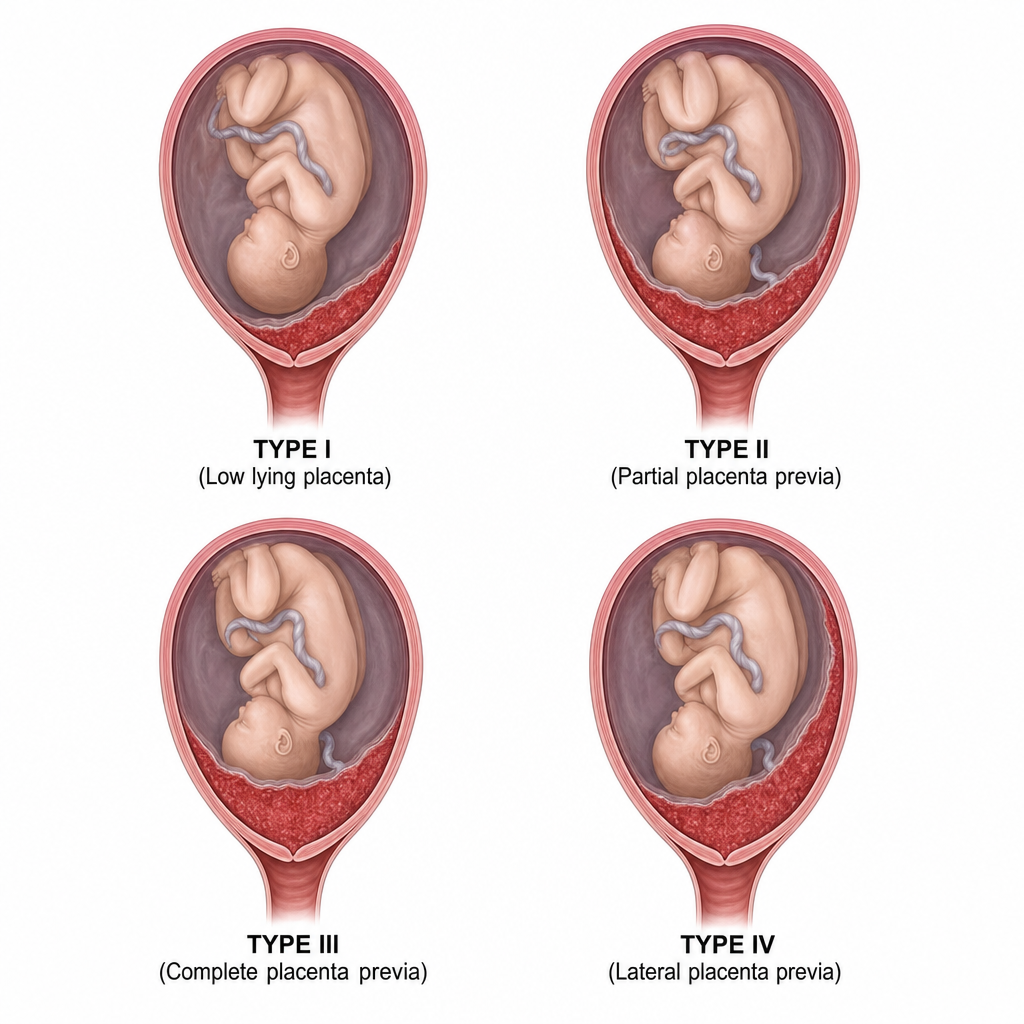
A transvaginal ultrasound performed at 28 weeks of gestation shows the placental edge reaching but not covering the internal cervical os. Based on the provided image, identify the type of placenta praevia.
A woman at 26 weeks of gestation presents for routine evaluation. On examination, fundal height corresponds to 24 weeks. Ultrasonography revealed decreased amniotic fluid. Which of the following conditions would have led to this presentation?
Chromosome number of partial hydatidiform mole is-
A patient with recurrent abortion is diagnosed to have antiphospholipid syndrome. What will be the treatment?
A female patient collapses soon after delivery. There is profuse bleeding and features of disseminated intravascular coagulation. Which of the following is the most likely etiology?
Practice by Chapter
Fetal Assessment Techniques
Practice Questions
Hypertensive Disorders in Pregnancy
Practice Questions
Intrauterine Growth Restriction
Practice Questions
Multiple Gestation
Practice Questions
Rh Isoimmunization and Other Blood Group Incompatibilities
Practice Questions
Intrauterine Fetal Therapy
Practice Questions
Prenatal Diagnosis and Genetic Counseling
Practice Questions
Placental Abnormalities
Practice Questions
Preterm Labor and Delivery
Practice Questions
Management of Medical Disorders in Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app