
Maternal-Fetal Medicine — MCQs

On this page
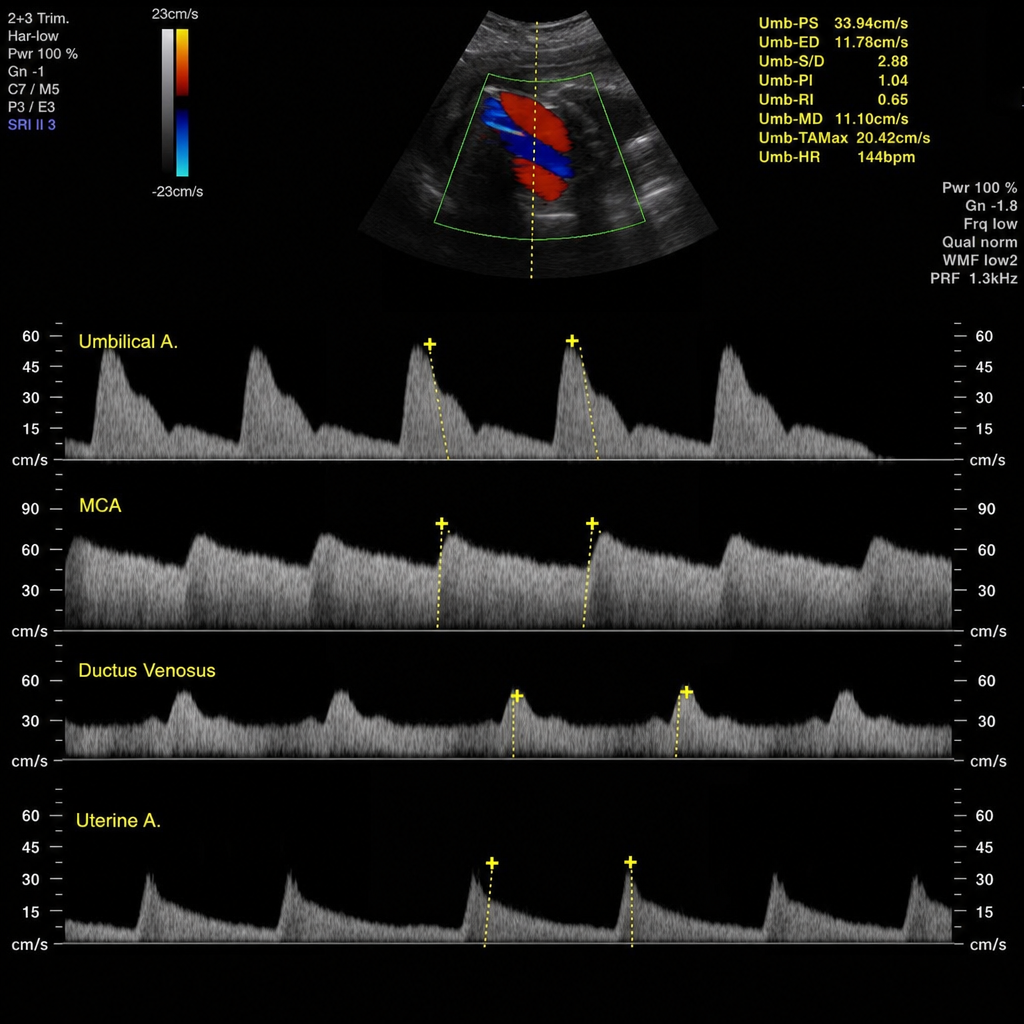
A 30-week pregnant female presents for antenatal Doppler assessment. Fetal biometry shows estimated fetal weight on the 8th centile. The umbilical artery Doppler shows absent end-diastolic flow (AEDF). The middle cerebral artery (MCA) PI is reduced at 1.1 (below the 5th centile), indicating brain-sparing. The ductus venosus shows reversal of the 'a' wave. The findings are shown. What is the recommended management?
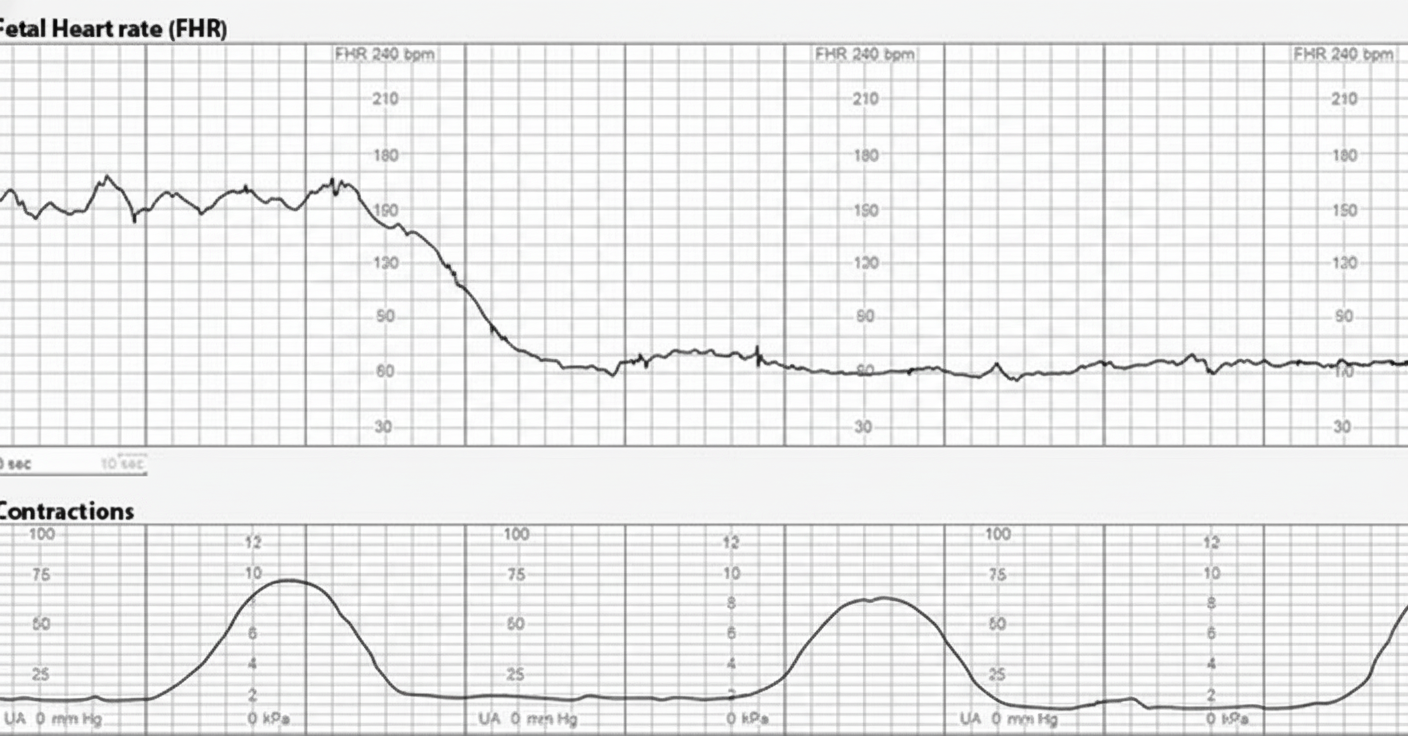
A 25-year-old woman, G2 P1 with a prior cesarean delivery, is in labor. She suddenly develops severe abdominal pain, and the uterine contractions cease. Vaginal bleeding is noted, and the fetal presenting part is no longer palpable at the cervix. The fetal heart rate monitor shows the tracing seen in the image, recorded just before the contractions ceased. What is your diagnosis?
Which one of the following is NOT a feature of severe pre-eclampsia?
A pregnant female with chronic hypertension whose blood pressure is controlled with antihypertensives should ideally be delivered at which gestational age?
A 30-week pregnant woman presents for an antenatal check-up complaining of mild dyspnea and palpitations. On examination, pedal edema is present. An ejection systolic murmur is noted. ECG shows sinus tachycardia, left axis deviation, and occasional premature ventricular beats. Echocardiogram reveals a small pleural effusion and mild mitral regurgitation. No other relevant findings are present. What is the next line of treatment?
A patient at 36 weeks of gestation presents with abdominal pain, uterine tenderness, and vaginal bleeding. Her vital signs are stable, and fetal heart tracing is regular. Which of the following steps is NOT required?
A G1 P0 patient presents with blood pressure of 160/102 mmHg, 3+ proteinuria, and right upper quadrant discomfort at 36 weeks gestation. Following induction of labor, she delivers vaginally and experiences 1500mL blood loss. Her serum creatinine rises from 0.98 mg/dL pre-delivery to 1.42 mg/dL post-delivery. What is the most likely diagnosis?
A woman with mitral stenosis but no pulmonary hypertension is in labor at 39 weeks of gestation. She has dyspnea on exertion and a pulse rate of 80 bpm. There are no basal crepitations in the lungs. The cervix is 4 cm dilated, and she is having 1-2 uterine contractions in 10 minutes. Which of the following steps is best avoided in her management?
A 36-year-old multigravida at 34 weeks gestation, with a history of two previous lower segment caesarean sections (LSCS), presents with an unstable lie. What is the most likely diagnosis in this case?
A 25-year-old nulliparous woman at 35 weeks' gestation presents with contractions, headache, and visual disturbances. Her pregnancy has been uncomplicated. Her temperature is 37 C, blood pressure is 160/110 mm Hg, pulse is 88/minute, and respirations are 12/minute. Examination reveals a cervix that is 2 cm dilated and 75% effaced, with contractions occurring every 2 minutes. Fetal heart rate is in the 140s and reactive. Urinalysis shows 3+ proteinuria. Laboratory values: leukocytes 9,400/mm3, hematocrit 35%, platelets 101,000/mm3, AST 200 U/L, and ALT 300 U/L. What is the most appropriate next step in management?
Practice by Chapter
Fetal Assessment Techniques
Practice Questions
Hypertensive Disorders in Pregnancy
Practice Questions
Intrauterine Growth Restriction
Practice Questions
Multiple Gestation
Practice Questions
Rh Isoimmunization and Other Blood Group Incompatibilities
Practice Questions
Intrauterine Fetal Therapy
Practice Questions
Prenatal Diagnosis and Genetic Counseling
Practice Questions
Placental Abnormalities
Practice Questions
Preterm Labor and Delivery
Practice Questions
Management of Medical Disorders in Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app