
Maternal-Fetal Medicine — MCQs

On this page
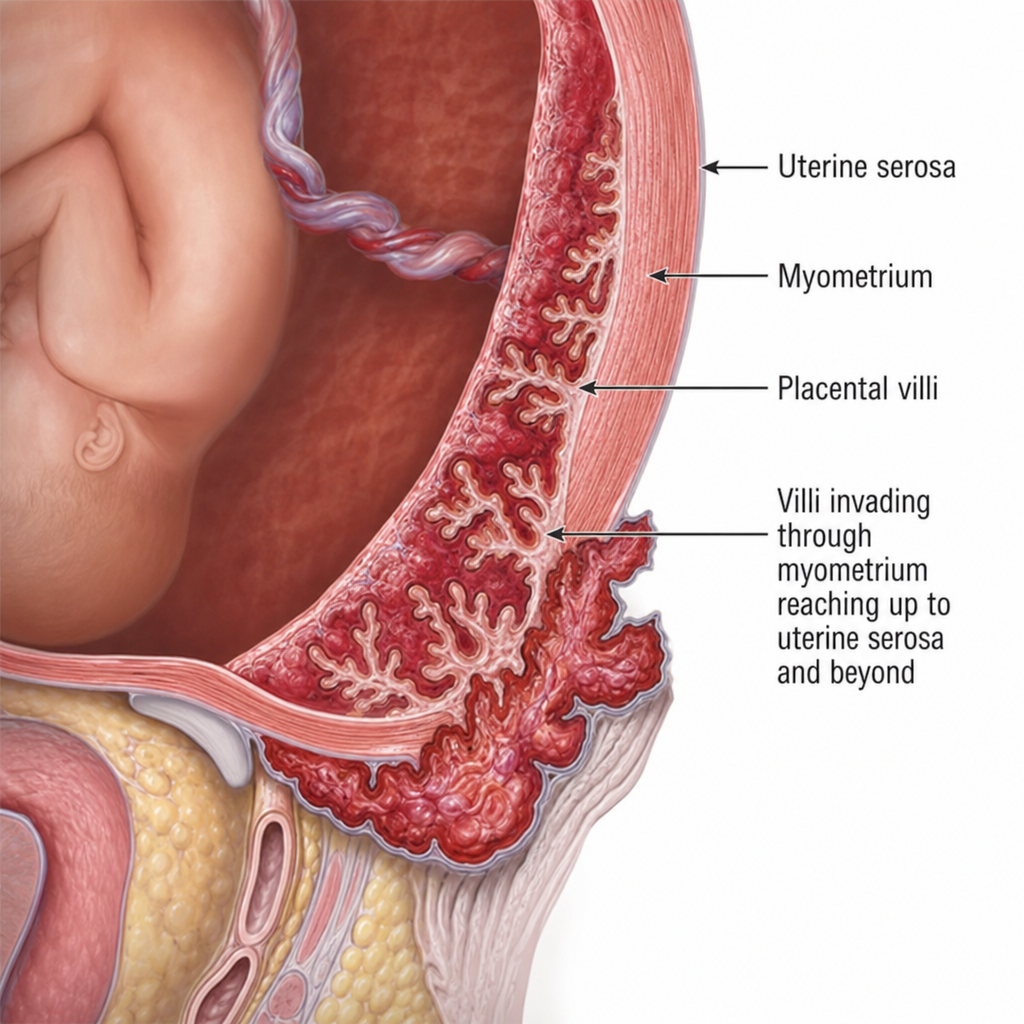
What does the below diagram indicate?
McDonald stitch is applied in the following conditions except:
Possibility of vertical transfer of HIV infection if no prophylaxis is given:
Which of the following statements is true regarding cerclage?
Ring of fire on USG signifies-
A 30-year-old lady develops retention of urine in the 2nd trimester. The most probable cause is:
Termination of pregnancy in placenta previa is indicated in: a) Active bleeding b) Active labour c) Gestational age > 34 weeks with live fetus d) Fetal malformation e) Unstable lie
A 30-year-old G2P1 is undergoing an elective repeat caesarean section at term. The infant is delivered without any difficulties, but the placenta cannot be removed easily because a clear plane between the placenta and uterine wall cannot be identified. The placenta is removed in pieces. This is followed by uterine atony and haemorrhage. All of the following are true regarding the condition except:
A 19-year-old woman presents to the emergency department reporting that she fainted at work earlier in the day. She has mild vaginal bleeding and her abdomen is diffusely tender and distended. She also complains of shoulder and abdominal pain. Her vital signs show temperature 97.6°F (36.4°C), pulse 120/min, and blood pressure 96/50 mmHg. To confirm the diagnosis suggested by the available clinical data, the best initial diagnostic procedure is
Risk for postnatal urinary abnormality is severe if Renal pelvic dilatation is ----- in third trimester?
Practice by Chapter
Fetal Assessment Techniques
Practice Questions
Hypertensive Disorders in Pregnancy
Practice Questions
Intrauterine Growth Restriction
Practice Questions
Multiple Gestation
Practice Questions
Rh Isoimmunization and Other Blood Group Incompatibilities
Practice Questions
Intrauterine Fetal Therapy
Practice Questions
Prenatal Diagnosis and Genetic Counseling
Practice Questions
Placental Abnormalities
Practice Questions
Preterm Labor and Delivery
Practice Questions
Management of Medical Disorders in Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app