
Maternal-Fetal Medicine — MCQs

On this page
A woman at 30 weeks of gestation is diagnosed with deep vein thrombosis (DVT). Which of the following is the most appropriate treatment for this patient?
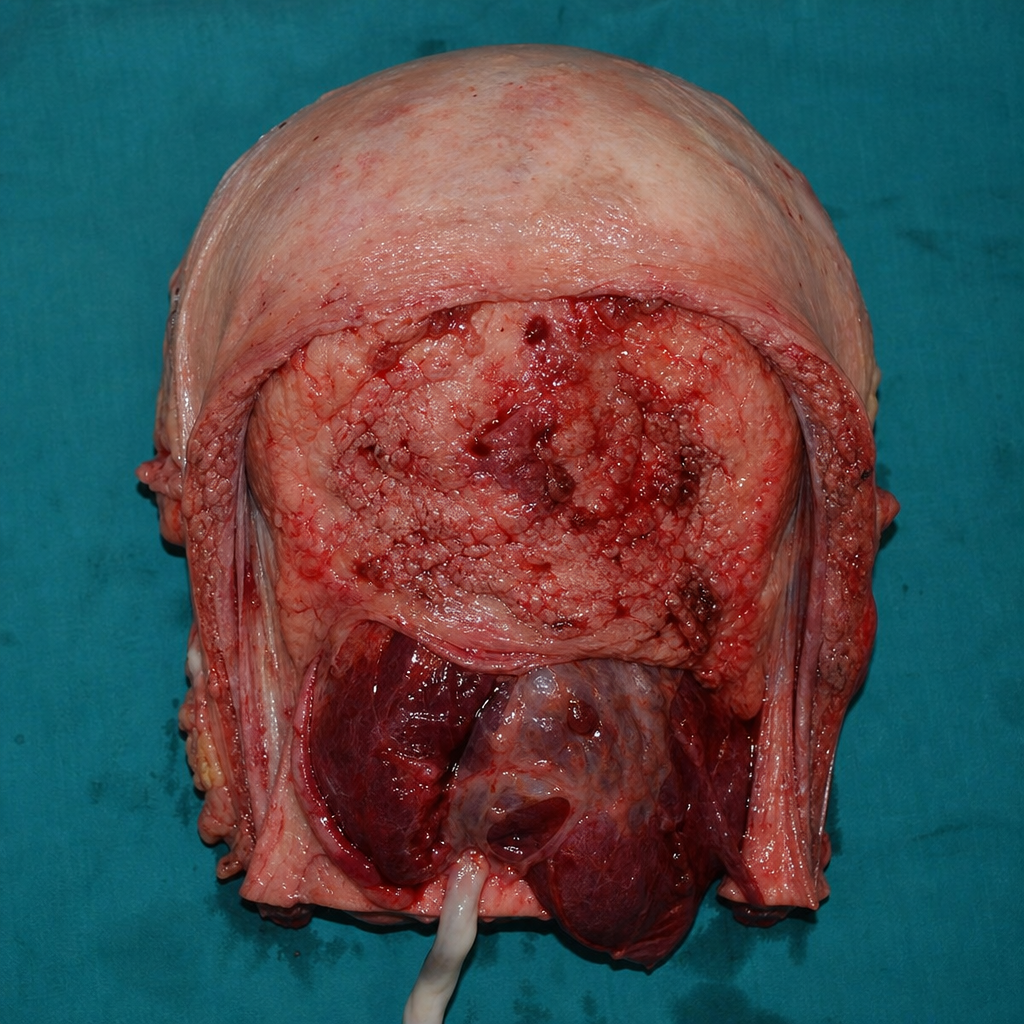
A G2P1L1 woman with a history of previous cesarean section presents with complications related to the placenta. The image below shows the gross appearance of the uterus with abnormal placental attachment to the uterine wall, with a cross-sectional view demonstrating chorionic villi adherent to the superficial myometrium without invasion through the full thickness of the uterine wall. What is the most likely diagnosis?
A woman presents with a history of recurrent abortions at 8,11 , and 22 weeks, with normal fetal cardiac activity in all three pregnancies. She also has a history of preeclampsia in her last pregnancy. What is the most probable cause?
A woman with eclampsia is started on magnesium sulfate. What is the first sign of magnesium sulfate toxicity?
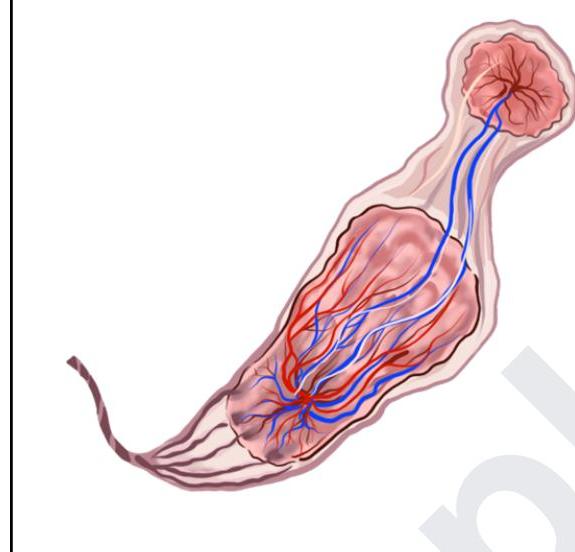
The given image depicts:
Which of the following is not true about lupus nephritis in pregnancy?
A 30-year-old pregnant female diagnosed with fibroid presented with fever, mild leukocytosis, and pain at 28 weeks. What is the likely cause?
Least chance of perinatal transmission?
All are the causes of non-immune hydrops except?
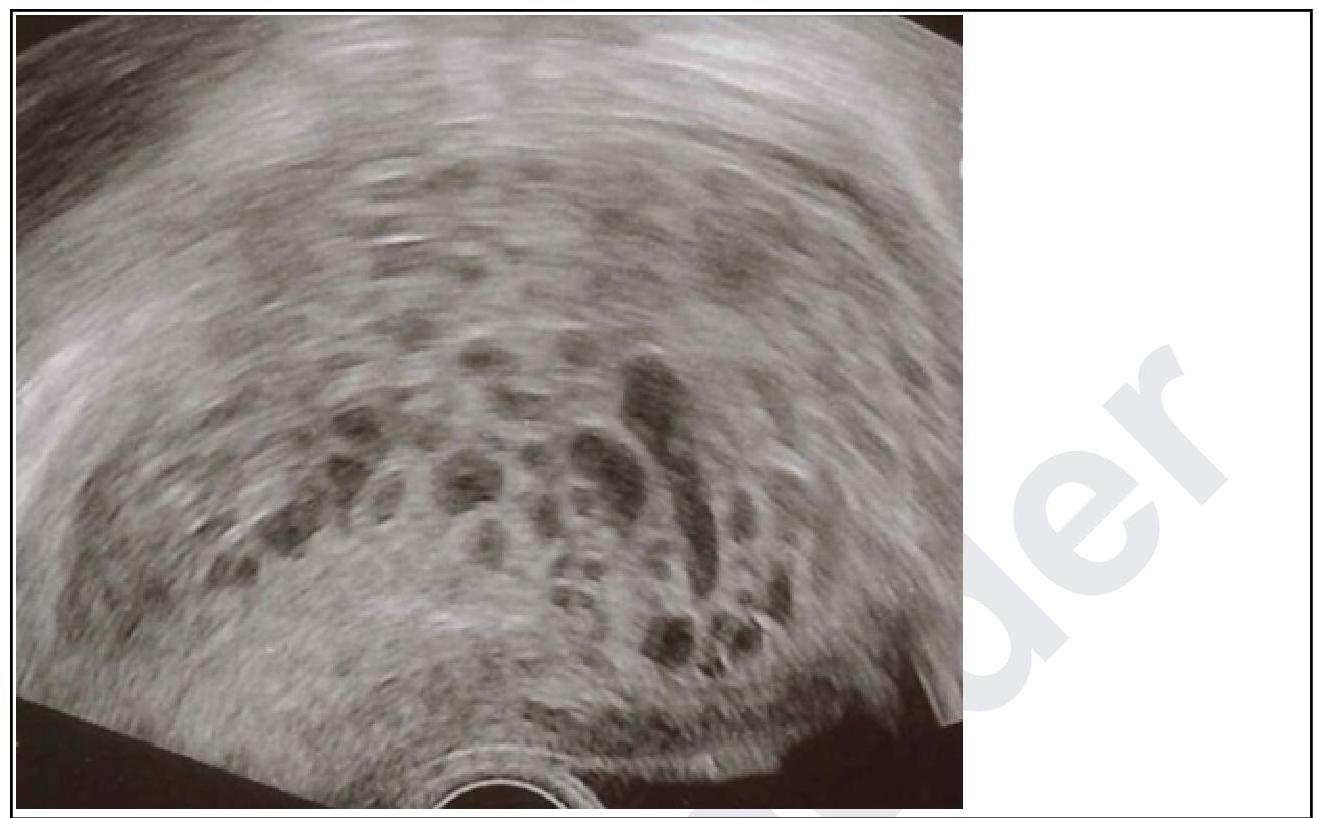
A primigravida in her 10th week of gestation presents with spotting. On examination, the uterus corresponds to 12 weeks. Transvaginal ultrasound was done and it is given below. What is your diagnosis?
Practice by Chapter
Fetal Assessment Techniques
Practice Questions
Hypertensive Disorders in Pregnancy
Practice Questions
Intrauterine Growth Restriction
Practice Questions
Multiple Gestation
Practice Questions
Rh Isoimmunization and Other Blood Group Incompatibilities
Practice Questions
Intrauterine Fetal Therapy
Practice Questions
Prenatal Diagnosis and Genetic Counseling
Practice Questions
Placental Abnormalities
Practice Questions
Preterm Labor and Delivery
Practice Questions
Management of Medical Disorders in Pregnancy
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app