
Labor and Delivery — MCQs

On this page
The normal rate of dilatation of the cervix in a primigravida in the active phase of labor is
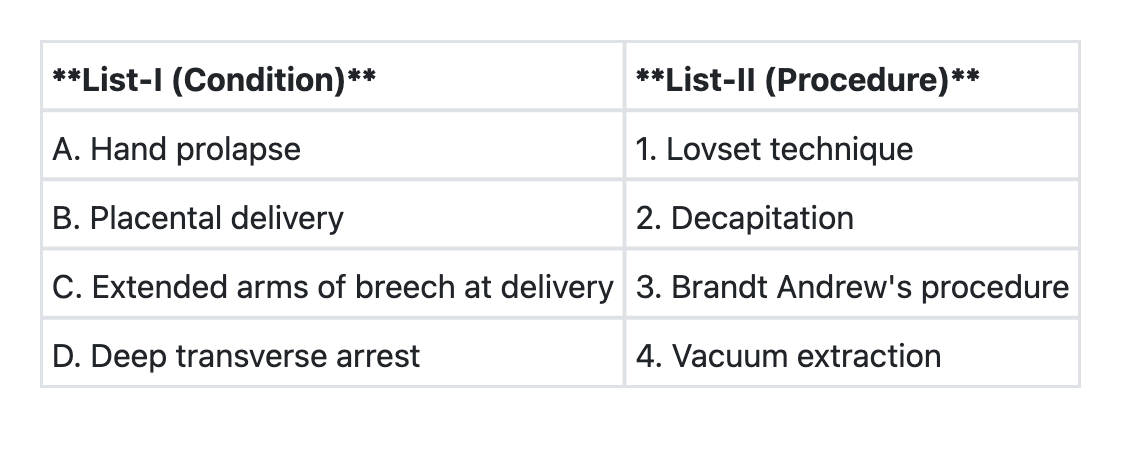
Match List-I with List-II and select the correct answer using the code given below the Lists:
A patient who just delivered at home presents with a third degree perineal tear. You will do the repair:
Face to pubes delivery occurs in which of the foetal position?
A G 2 P 1 A 0 presents with full term pregnancy with transverse lie in the first stage of labour. On examination, cervix is 5 cm dilated, membranes are intact and foetal heart sounds are regular. The appropriate management would be:
Which of the following methods for induction of labour should not be used in the patient with previous lower segment caesarean section?
Which one of the following is not a complication of shoulder dystocia?
Immediately after third stage of labour in a case of full term delivery, the fundus of the uterus is:
A 20 year old primigravida is admitted with full term pregnancy and labour pains. At 4 A.M. she goes into active phase of labour with 4 cm cervical dilatation. Membranes rupture during p/v examination showing clear liquor. A repeat p/v after 4 hours of good uterine contractions reveals a cervical dilatation of 5 cm. What should be the next step in management?
Which one of the following is not a suitable condition for outlet forceps application?
Practice by Chapter
Physiology of Labor
Practice Questions
Stages of Labor and Normal Progression
Practice Questions
Fetal Monitoring Techniques
Practice Questions
Pain Management in Labor
Practice Questions
Induction and Augmentation of Labor
Practice Questions
Operative Delivery (Forceps and Vacuum)
Practice Questions
Cesarean Section: Indications and Techniques
Practice Questions
Dystocia and Abnormal Labor Patterns
Practice Questions
Obstetric Emergencies
Practice Questions
Postpartum Hemorrhage Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app