
Labor and Delivery — MCQs

On this page
Shoulder dystocia is diagnosed when the anterior shoulder fails to deliver after what time following delivery of the head?
In which of the following cases is the drug below contraindicated?
In a primigravida what is a satisfactory dilation rate?
All of the following are true about audit in obstetrics except:
A 28-year-old primigravida at 38 weeks gestation presents in active labor. Fetal heart rate monitoring shows variable decelerations with each contraction. Cervix is 6 cm dilated, and the umbilical cord is palpable alongside the presenting part. What is the most appropriate immediate management?
In managing shoulder dystocia during vaginal delivery, which of the following is the correct sequence of maneuvers?
A 32-year-old G2P1 woman with a previous cesarean section is undergoing a trial of vaginal delivery at 39 weeks. She is in active labor with 8 cm cervical dilation and fetal station at -1. Continuous fetal monitoring reveals fetal bradycardia, and maternal pulse is 110/min. What is the most appropriate next step in management?
A 38-week pregnant woman in active labor with 5 cm cervical dilatation and regular contractions suddenly develops umbilical cord prolapse. What is the most appropriate immediate management?
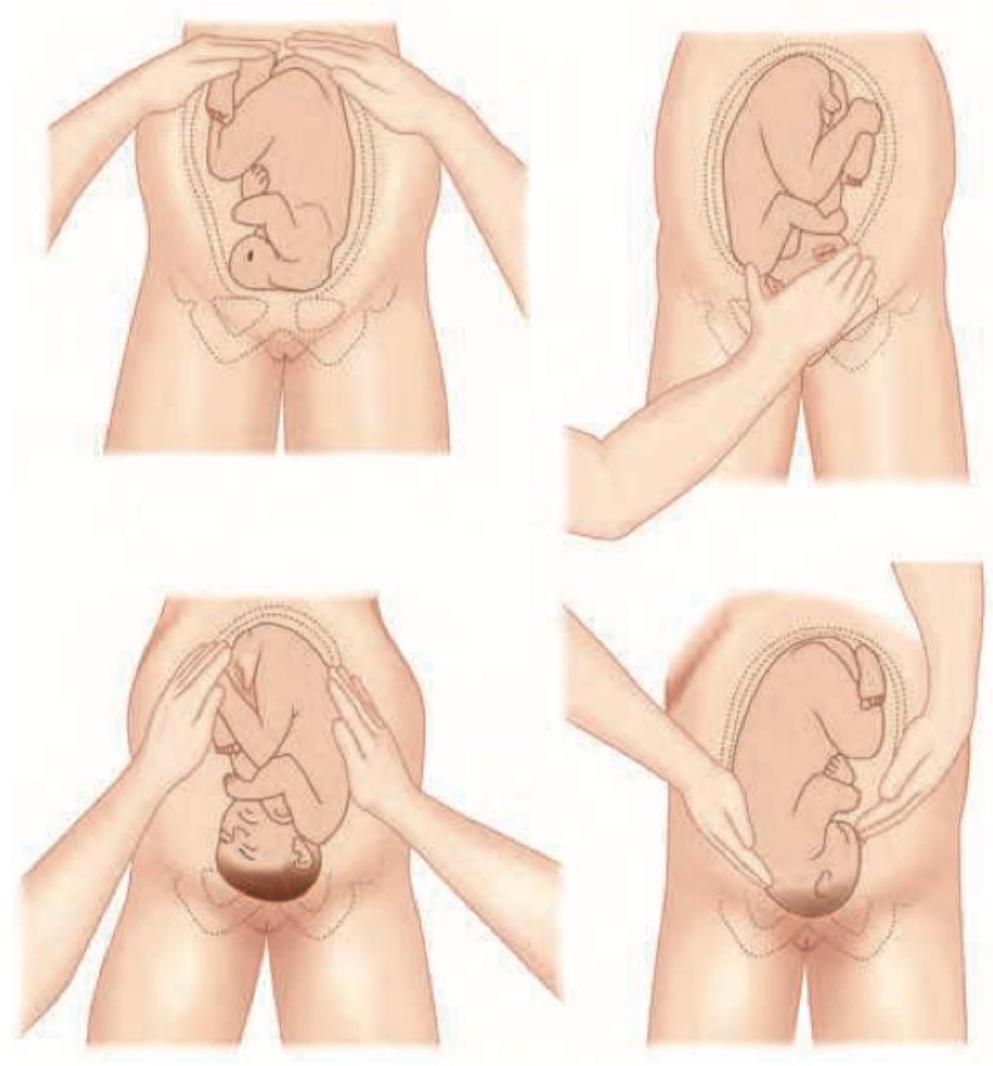
Identify the maneuver shown in the image.
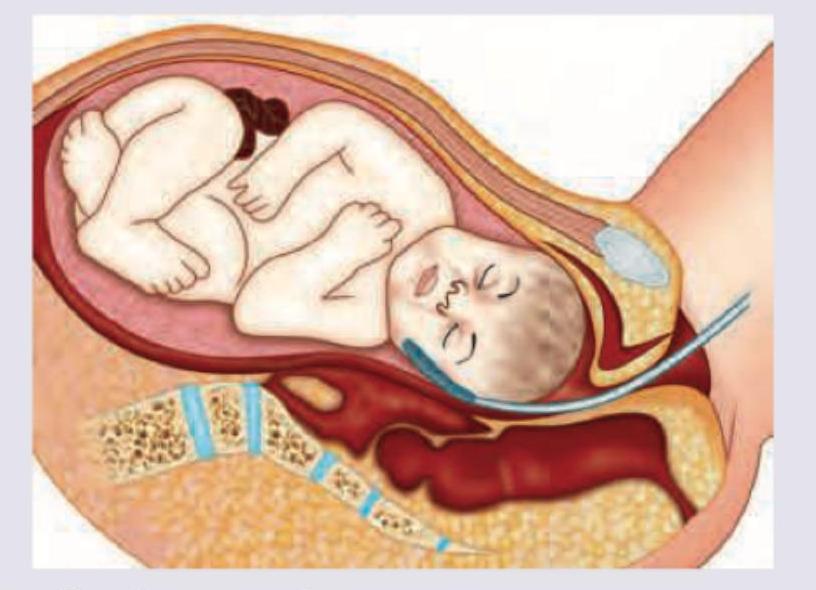
Which technique of intrapartum fetal monitoring is shown here?
Practice by Chapter
Physiology of Labor
Practice Questions
Stages of Labor and Normal Progression
Practice Questions
Fetal Monitoring Techniques
Practice Questions
Pain Management in Labor
Practice Questions
Induction and Augmentation of Labor
Practice Questions
Operative Delivery (Forceps and Vacuum)
Practice Questions
Cesarean Section: Indications and Techniques
Practice Questions
Dystocia and Abnormal Labor Patterns
Practice Questions
Obstetric Emergencies
Practice Questions
Postpartum Hemorrhage Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app