
Labor and Delivery — MCQs

On this page
Which of the following is NOT related to blood coagulation disorders in obstetrics?
Saffron colored meconium is seen in which condition?
Combination of Nifedipine with what other tocolytic agent can potentially cause dangerous neuromuscular blockade?
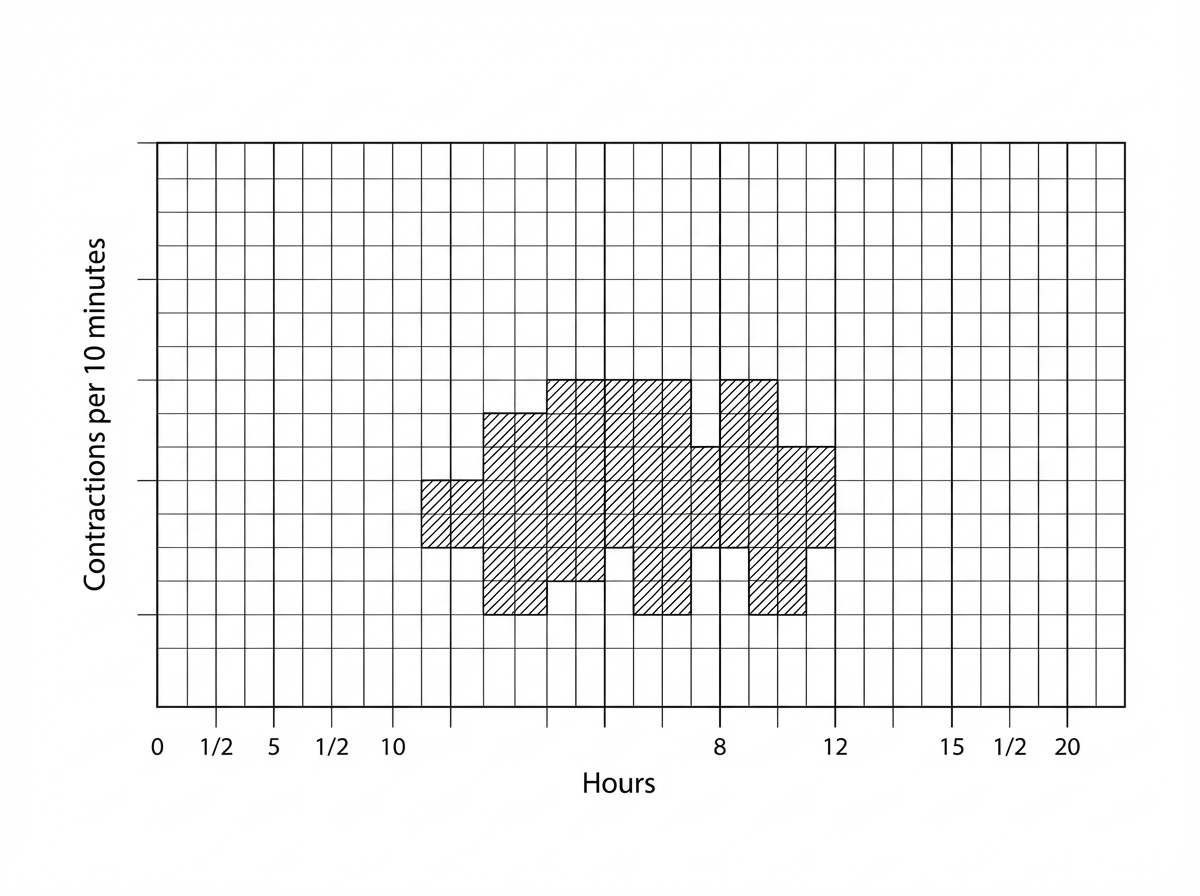
What does the indicator in the following partograph signify?
An early deceleration pattern on cardiotocography indicates what?
Pain in early labor is transmitted through which spinal nerve segments?
Prolonged latent phase of labor is commonly seen in which of the following conditions?
In twin pregnancy, vaginal delivery is contraindicated in which of the following conditions?
Antepartum hemorrhage occurs after how many weeks of gestation?
Prelabour pains are mediated through which spinal nerve roots?
Practice by Chapter
Physiology of Labor
Practice Questions
Stages of Labor and Normal Progression
Practice Questions
Fetal Monitoring Techniques
Practice Questions
Pain Management in Labor
Practice Questions
Induction and Augmentation of Labor
Practice Questions
Operative Delivery (Forceps and Vacuum)
Practice Questions
Cesarean Section: Indications and Techniques
Practice Questions
Dystocia and Abnormal Labor Patterns
Practice Questions
Obstetric Emergencies
Practice Questions
Postpartum Hemorrhage Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app