
Labor and Delivery — MCQs

On this page
What is the management for occipitoposterior position in labor?
All are features of fetal distress except?
What is the best management for a mento-posterior presentation during labor?
Cord prolapse is most commonly associated with which of the following conditions?
A pregnant lady has delivered a baby 35 minutes back. However, the placenta has not been delivered. What is the next line of management?
All of the following are true of placenta previa except?
Forceps may be applied for delivery for all situations listed below, EXCEPT?
What is the transverse diameter of the female mid-pelvic plane?
A pregnant lady in her first trimester presents with vaginal bleeding. On examination, the os is closed and uterine size corresponds to the period of amenorrhoea. What is the most likely diagnosis?
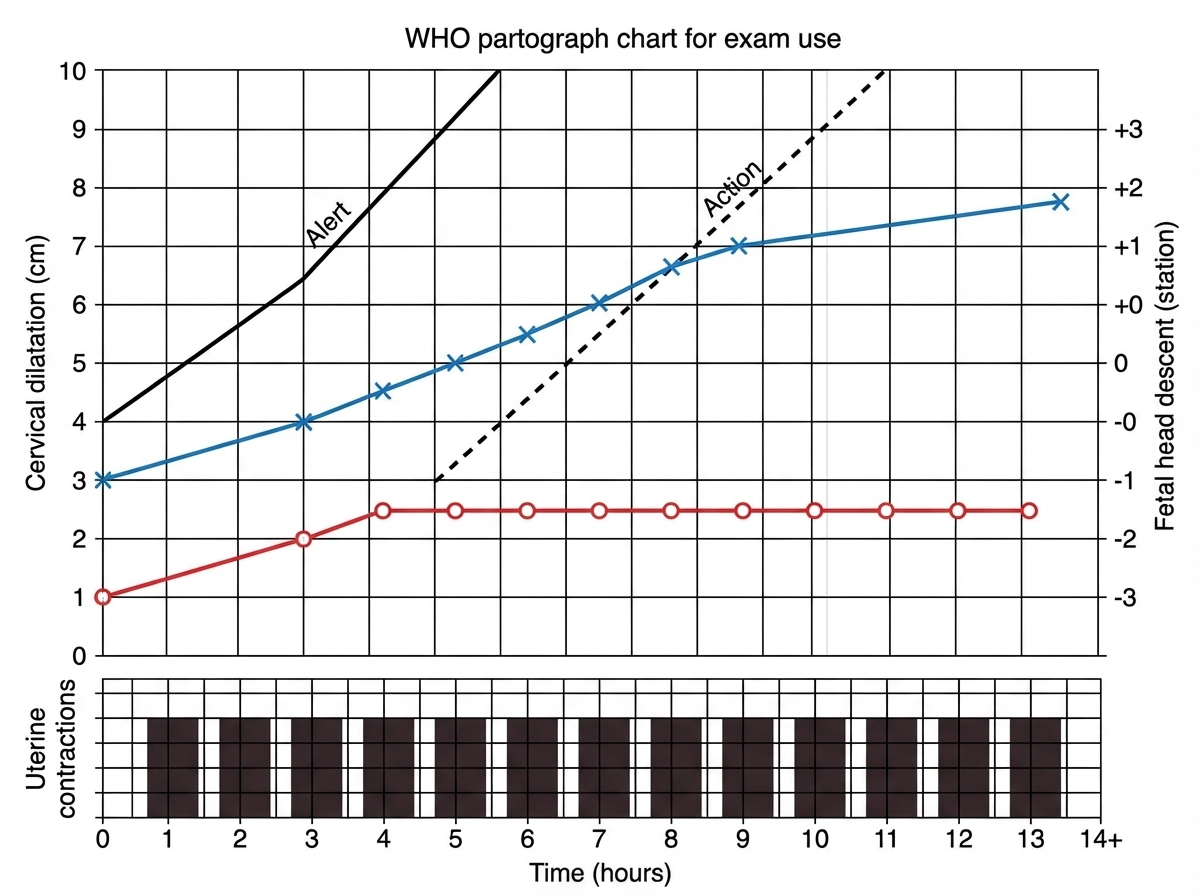
Interpret the given partogram:
Practice by Chapter
Physiology of Labor
Practice Questions
Stages of Labor and Normal Progression
Practice Questions
Fetal Monitoring Techniques
Practice Questions
Pain Management in Labor
Practice Questions
Induction and Augmentation of Labor
Practice Questions
Operative Delivery (Forceps and Vacuum)
Practice Questions
Cesarean Section: Indications and Techniques
Practice Questions
Dystocia and Abnormal Labor Patterns
Practice Questions
Obstetric Emergencies
Practice Questions
Postpartum Hemorrhage Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app