
Labor and Delivery — MCQs

On this page
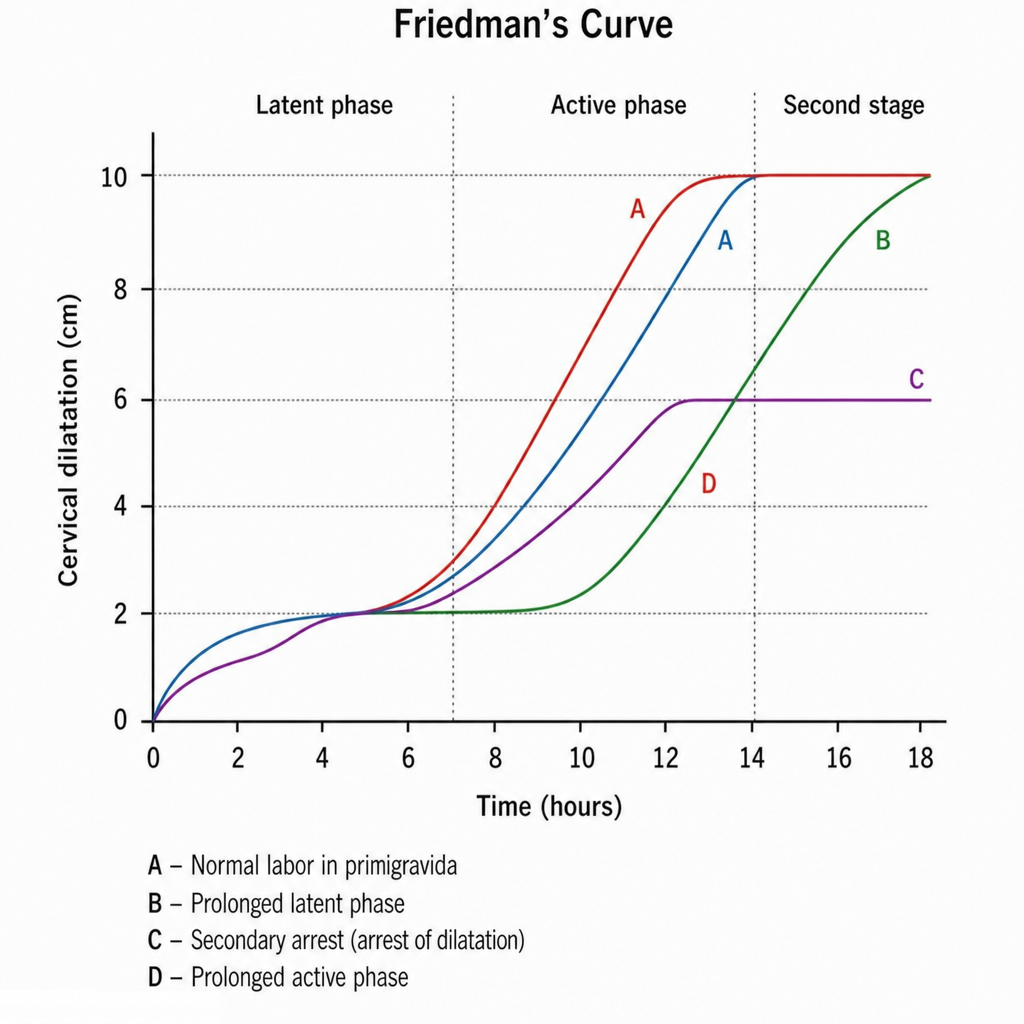
The provided graph illustrates the stages of labor. Which statement is true regarding graph C?
Early cord clamping is indicated in all except?
What is the engaging diameter if the vertex is markedly deflexed?
Which of the following features can be used to define a contracted pelvis?
In a brow presentation, what is the typical position of the fetal head?
In intrapartum fetal monitoring of women with pregnancies at risk, fetal auscultation is performed at least every --- minutes during the first stage of labor and every --- minutes during the second stage?
Compared with a normally shaped placenta, which complication of third-stage labor is more common with a succenturiate lobe?
A 37-week pregnant female presents with mild labor pain for 10 hours. On examination, the cervix is persistently 1 cm dilated and non-effaced. What is the next appropriate management?
A 39-week gestation patient presents with a footling presentation. What is the most appropriate management?
Successful trial of labour can be expected in:
Practice by Chapter
Physiology of Labor
Practice Questions
Stages of Labor and Normal Progression
Practice Questions
Fetal Monitoring Techniques
Practice Questions
Pain Management in Labor
Practice Questions
Induction and Augmentation of Labor
Practice Questions
Operative Delivery (Forceps and Vacuum)
Practice Questions
Cesarean Section: Indications and Techniques
Practice Questions
Dystocia and Abnormal Labor Patterns
Practice Questions
Obstetric Emergencies
Practice Questions
Postpartum Hemorrhage Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app