
Labor and Delivery — MCQs

On this page
What is the most common position of engagement in vertex presentation?
A multigravida patient with a 4 kg fetus has been in labor for 15 hours, with cervical dilation at 5 cm for the last 8 hours. What is the most appropriate management for this patient?
What is the presenting diameter of a fully flexed head?
A 41-week pregnant female, confirmed by radiological investigation and very sure of her last menstrual period, presents with no uterine contractions, no effacement, and no dilatation. Which of the following should not be administered?
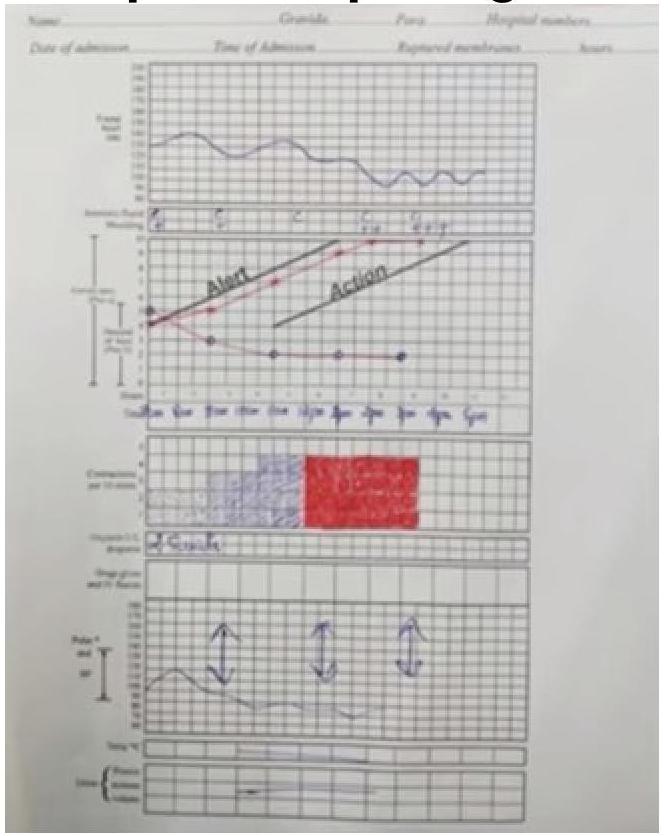
Given the following partogram data, what does a cervical dilation curve to the right of the alert line indicate?
A primigravida presents to the labor room at 40 weeks of gestation with lower abdominal pain. She has been in labor for 3 hours. Which of the following will determine if she is in active labor?
Which of these steps is followed first for the management of shoulder dystocia after McRoberts maneuver?
Which of the following describes the points marked in the diagram of pelvic measurements?

There is overlapping of skull sutures which can be reduced with gentle pressure. What is the grade of moulding?
When the fetus is at station +2 and the fetal skull reaches the pelvic floor, which of the following statements is MOST clinically relevant?
Practice by Chapter
Physiology of Labor
Practice Questions
Stages of Labor and Normal Progression
Practice Questions
Fetal Monitoring Techniques
Practice Questions
Pain Management in Labor
Practice Questions
Induction and Augmentation of Labor
Practice Questions
Operative Delivery (Forceps and Vacuum)
Practice Questions
Cesarean Section: Indications and Techniques
Practice Questions
Dystocia and Abnormal Labor Patterns
Practice Questions
Obstetric Emergencies
Practice Questions
Postpartum Hemorrhage Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app