
Labor and Delivery — MCQs

On this page
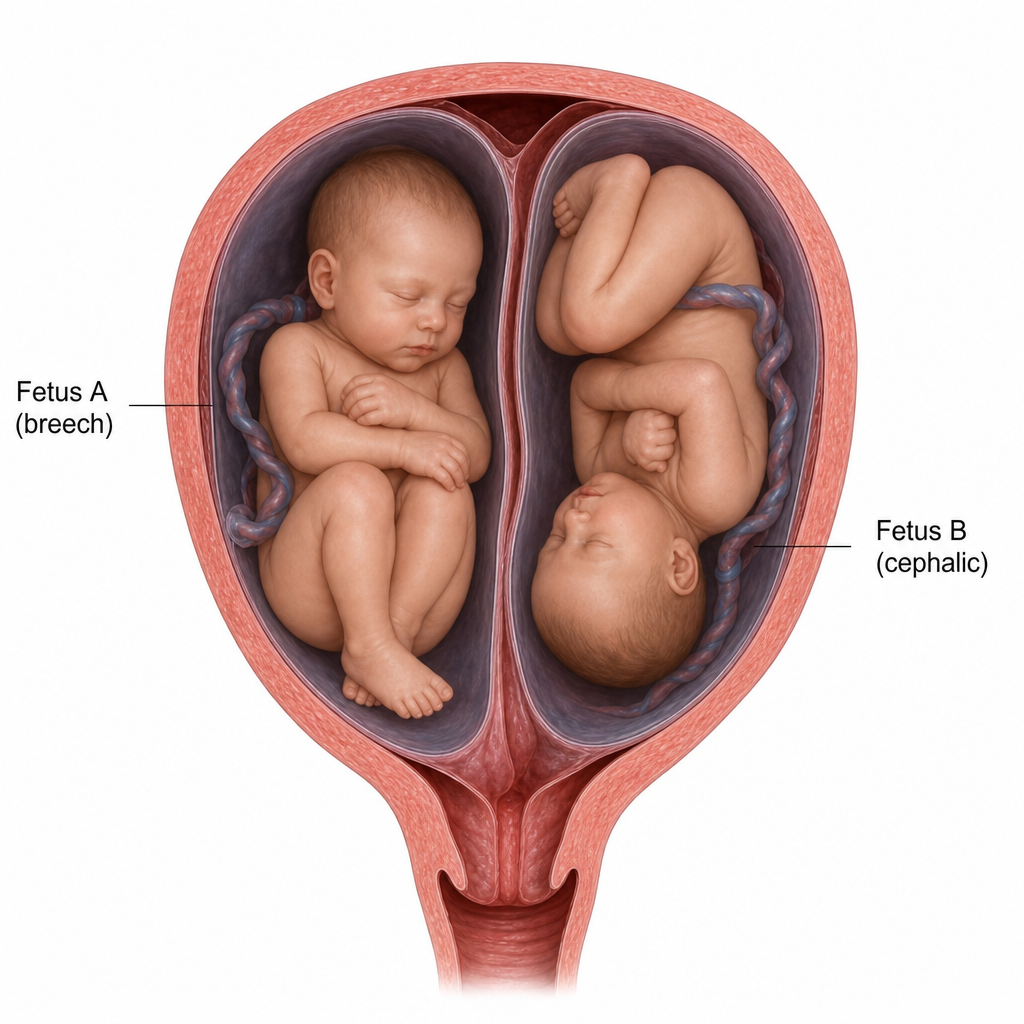
In the image showing twin pregnancy where fetus A (first twin) is in breech presentation and fetus B (second twin) is in cephalic presentation, what is the recommended method of delivery for fetuses A and B respectively?
A patient presents with infraumbilical flattening and the fetal heart rate is heard laterally. What is the most likely fetal position?
A pregnant female presents with active herpetic lesions on the vulva. What is the most appropriate management?
After delivering a baby boy, a 25 -year-old mother developed acute PPH and hypovolemic shock, and major blood transfusion occurred. All of the following are complications of blood transfusion except?
A primigravida is in labor. Her per-vaginal examination revealed a posterior cervix with 5 cm cervical length, 1 cm dilatation, soft consistency, and head at -1 station. Calculate the Bishop score.
Which of the following is a part of AMTSL?
After a normal delivery in a 27-year-old female, placenta is still attached to the uterus. Most common complication which can occur due to forceful traction of cord?
32 years old lady with twin dichorionic diamniotic pregnancy, first baby breech presentation and second baby cephalic presentation. What is the management?
Among the following the plane of least pelvic dimension is:
A primipara is in labor and an episiotomy is about to be cut. Compared with a midline episiotomy, an advantage of mediolateral episiotomy is
Practice by Chapter
Physiology of Labor
Practice Questions
Stages of Labor and Normal Progression
Practice Questions
Fetal Monitoring Techniques
Practice Questions
Pain Management in Labor
Practice Questions
Induction and Augmentation of Labor
Practice Questions
Operative Delivery (Forceps and Vacuum)
Practice Questions
Cesarean Section: Indications and Techniques
Practice Questions
Dystocia and Abnormal Labor Patterns
Practice Questions
Obstetric Emergencies
Practice Questions
Postpartum Hemorrhage Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app