
Labor and Delivery — MCQs

On this page
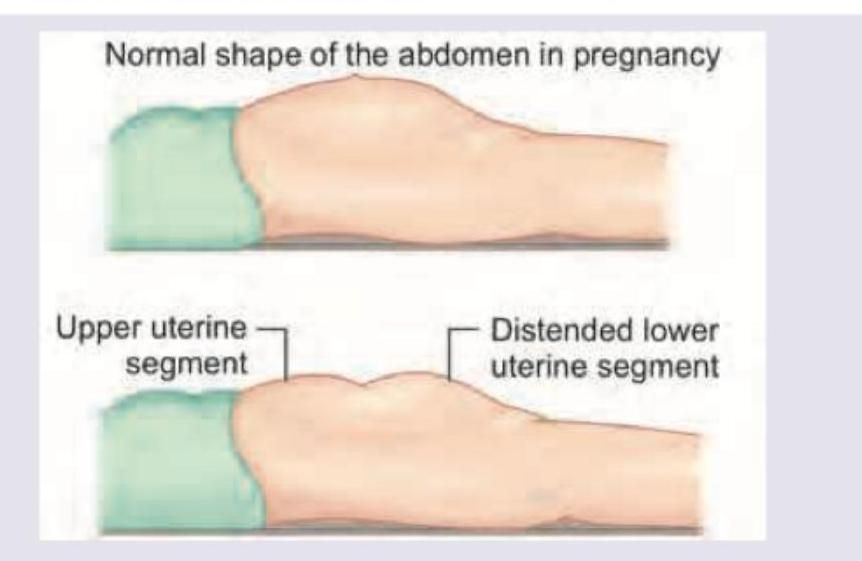
A 25-year-old primigravida has presented in obstructed labour. On examination she is exhausted and has a tender uterus with a groove felt per abdomen as shown in the image. Fetal parts are not felt. What is the diagnosis? (DNB Pattern 2018)
Which of the following factors favour posterior position of the vertex? I. Anthropoid pelvis II. Low inclination pelvis III. Attachment of placenta on the anterior wall IV. Primary brachycephaly Select the correct answer using the code given below :
Which of the following statements are correct regarding shoulder dystocia? I. It can be predicted during early labour. II. Fetal macrosomia is a risk factor. III. Turtle neck sign is present. IV. Episiotomy should always be given. Select the answer using the code given below :
According to WHO Intrapartum Care Guidelines 2018, which of the following are correct about birthing position? I. For a woman without epidural analgesia, adoption of birthing position is individual woman's choice. II. For a woman without epidural analgesia, upright birthing position may be adopted. III. For a woman with epidural analgesia, lithotomy and supine position only are recommended. Select the answer using the code given below :
According to WHO Intrapartum Care Guidelines 2018, which one of the following is correct about duration of first stage labour?
The Matthews Duncan process has been described for :
Which of the following factors are associated with cord prolapse during labour? I. Malpresentations II. Contracted pelvis III. Induction with engaged presenting part IV. Prematurity Select the correct answer using the code given below :
During delivery of HIV infected women, which of the following are recommended ? 1. Zidovudine (ZDV) is given at the onset of labour. 2. Elective caesarean delivery reduces the risk of vertical transmission. 3. Amniotomy and oxytocin augmentation should be done. 4. Antiretroviral therapy should be given to all neonates. Select the correct answer using the code given below :
Which of the following correctly defines the first stage of labor? 1. Full dilatation of cervix to the expulsion of the fetus from the birth canal 2. Maternal bearing down efforts and ends with the delivery of the baby 3. The onset of true labor pains and ends with the full dilatation of cervix 4. The formation of bag of waters
Secondary arrest of dilatation during the process of labour may be due to which of the following factors ? 1. Poor uterine contractions 2. Cessation of cervical dilatation despite strong uterine contractions 3. Disproportion and malpresentation Select the correct answer using the code given below :
Practice by Chapter
Physiology of Labor
Practice Questions
Stages of Labor and Normal Progression
Practice Questions
Fetal Monitoring Techniques
Practice Questions
Pain Management in Labor
Practice Questions
Induction and Augmentation of Labor
Practice Questions
Operative Delivery (Forceps and Vacuum)
Practice Questions
Cesarean Section: Indications and Techniques
Practice Questions
Dystocia and Abnormal Labor Patterns
Practice Questions
Obstetric Emergencies
Practice Questions
Postpartum Hemorrhage Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app