
Labor and Delivery — MCQs

On this page
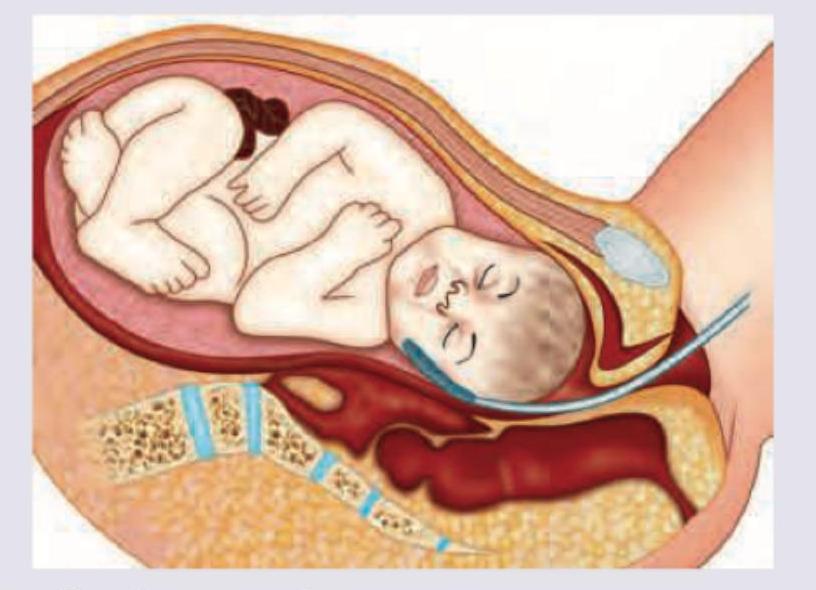
Which technique of intrapartum fetal monitoring is shown here?
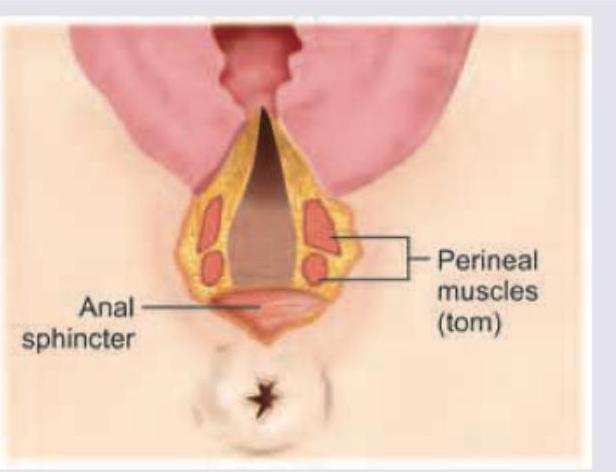
Which degree of obstetric anal sphincter injury is seen here?
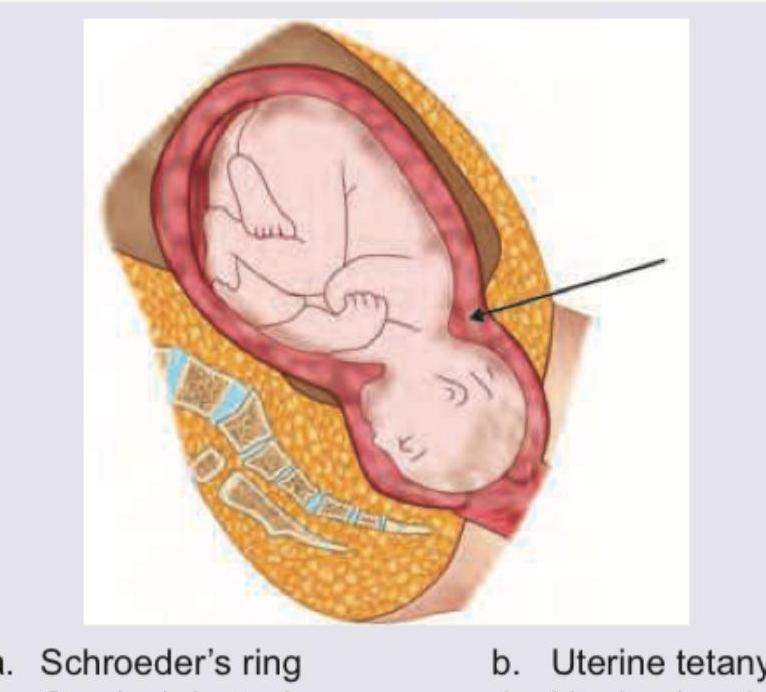
Which of the following causes of dysfunctional labour is shown below?
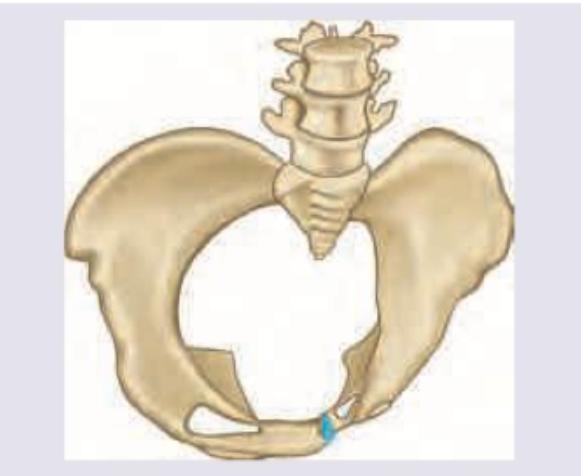
The following delivery is seen with which type of pelvis?
The image shows:
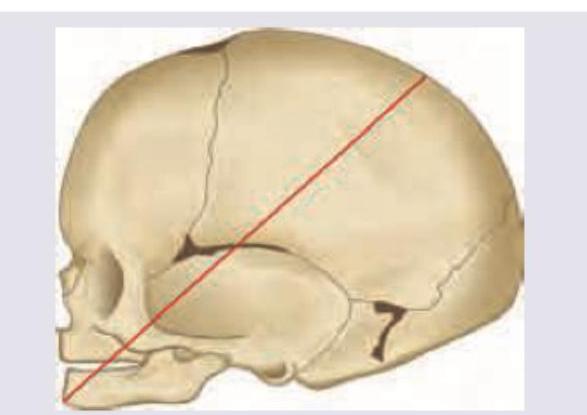
The following diameter is called \qquad and engages in \qquad presentation.
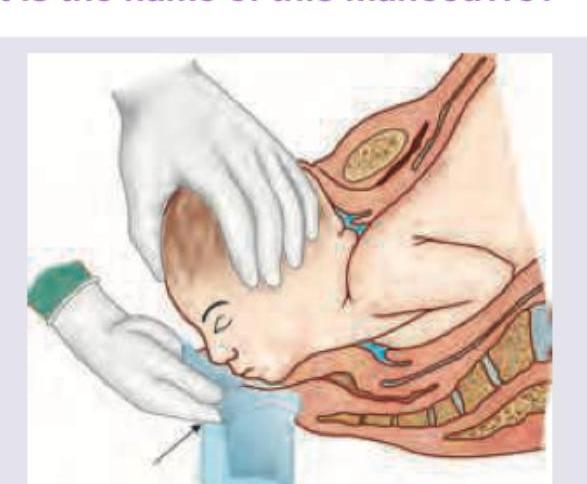
What is the name of this manoeuvre?
A 25-year-old primigravida at 38POG presents with painful uterine contractions and rupture of bag of water. On examination her cervix is 5 cm dilated and the malpresentation is as shown. Fetal heart rate tracing is reactive. Which of the following is the best method to achieve delivery?
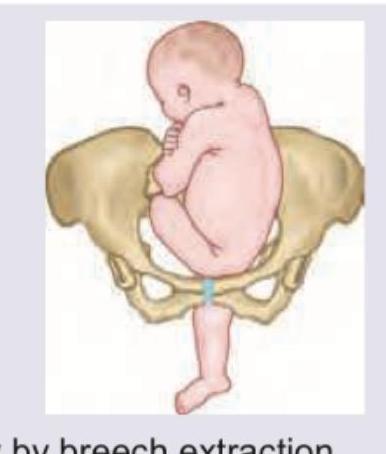
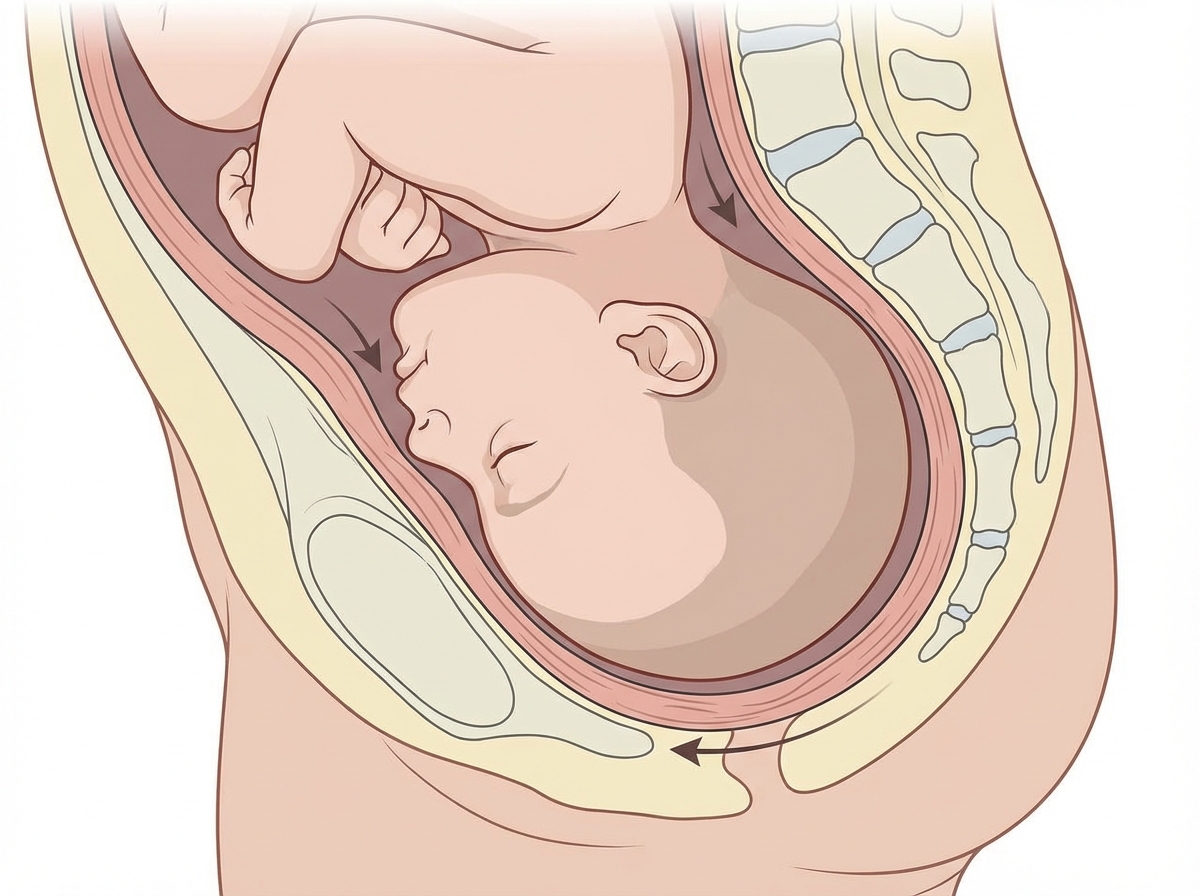
Identify the presentation shown below:

According to the Caldwell-Moloy classification, which of the following pelvic types is the LEAST common in women?
Practice by Chapter
Physiology of Labor
Practice Questions
Stages of Labor and Normal Progression
Practice Questions
Fetal Monitoring Techniques
Practice Questions
Pain Management in Labor
Practice Questions
Induction and Augmentation of Labor
Practice Questions
Operative Delivery (Forceps and Vacuum)
Practice Questions
Cesarean Section: Indications and Techniques
Practice Questions
Dystocia and Abnormal Labor Patterns
Practice Questions
Obstetric Emergencies
Practice Questions
Postpartum Hemorrhage Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app