
Labor and Delivery — MCQs

On this page
Battledore placenta is associated with the highest risk of which complication?
Active management of the third stage of labor is indicated for all of the following conditions EXCEPT?
Regarding precipitous labor, which of the following statements is FALSE?
All of the following drugs are effective for cervical ripening during pregnancy except:
Induction of labor at term is not indicated in which of the following conditions?
What is the risk of scar rupture in a previous lower segment cesarean section (LSCS)?
In which of the following patients can a midline episiotomy be considered superior to a mediolateral episiotomy during delivery of the fetus?
Combination of Nifedipine with what other tocolytic agent can potentially cause dangerous neuromuscular blockade?
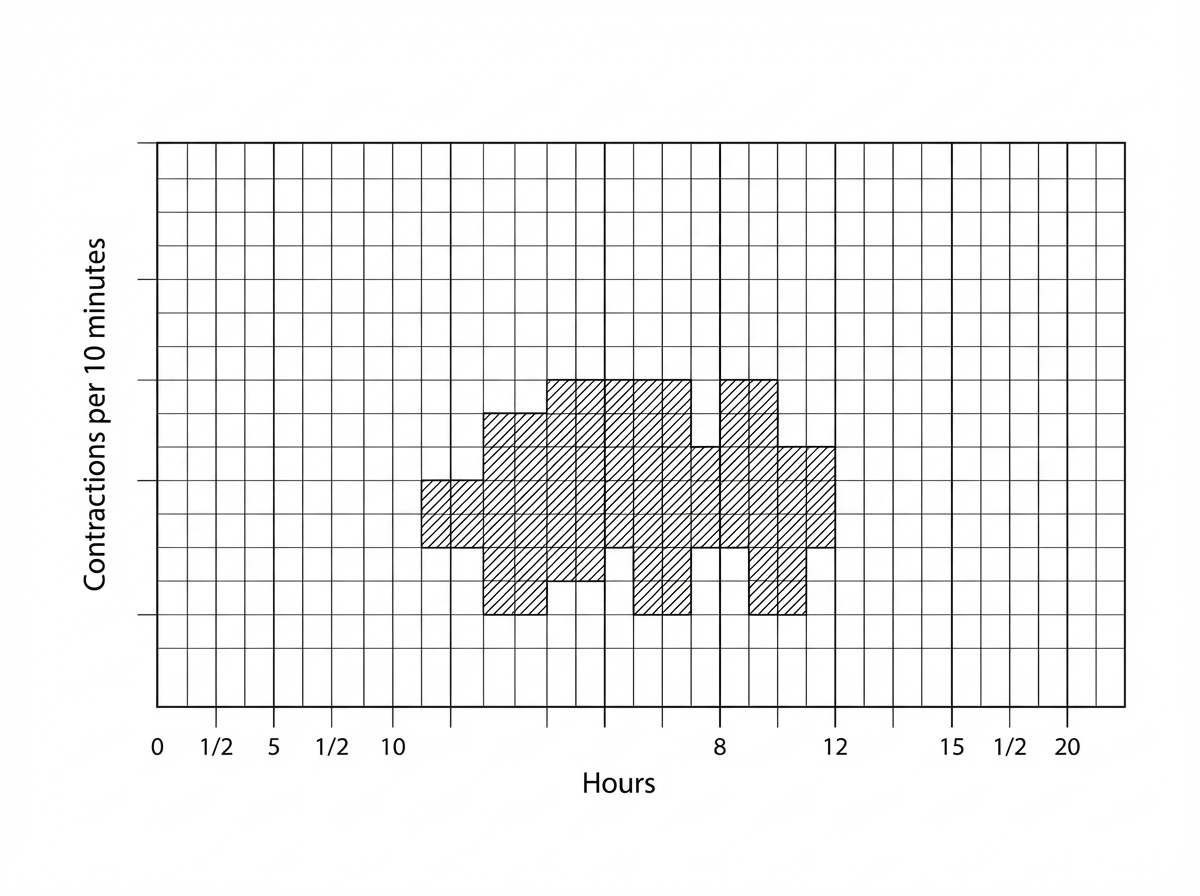
What does the indicator in the following partograph signify?
Prolonged latent phase of labor is commonly seen in which of the following conditions?
Practice by Chapter
Physiology of Labor
Practice Questions
Stages of Labor and Normal Progression
Practice Questions
Fetal Monitoring Techniques
Practice Questions
Pain Management in Labor
Practice Questions
Induction and Augmentation of Labor
Practice Questions
Operative Delivery (Forceps and Vacuum)
Practice Questions
Cesarean Section: Indications and Techniques
Practice Questions
Dystocia and Abnormal Labor Patterns
Practice Questions
Obstetric Emergencies
Practice Questions
Postpartum Hemorrhage Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app