
Labor and Delivery — MCQs

On this page
A pregnant lady has delivered a baby 35 minutes back. However, the placenta has not been delivered. What is the next line of management?
A 26-year-old G3P2L2 at 40 weeks presents in the second stage of labor. The baby's head delivers spontaneously, but then retracts back against the perineum. Even with downward traction, the baby's anterior shoulder fails to deliver. All of the following are appropriate next steps in the management of this patient EXCEPT?
What is the transverse diameter of the female mid-pelvic plane?
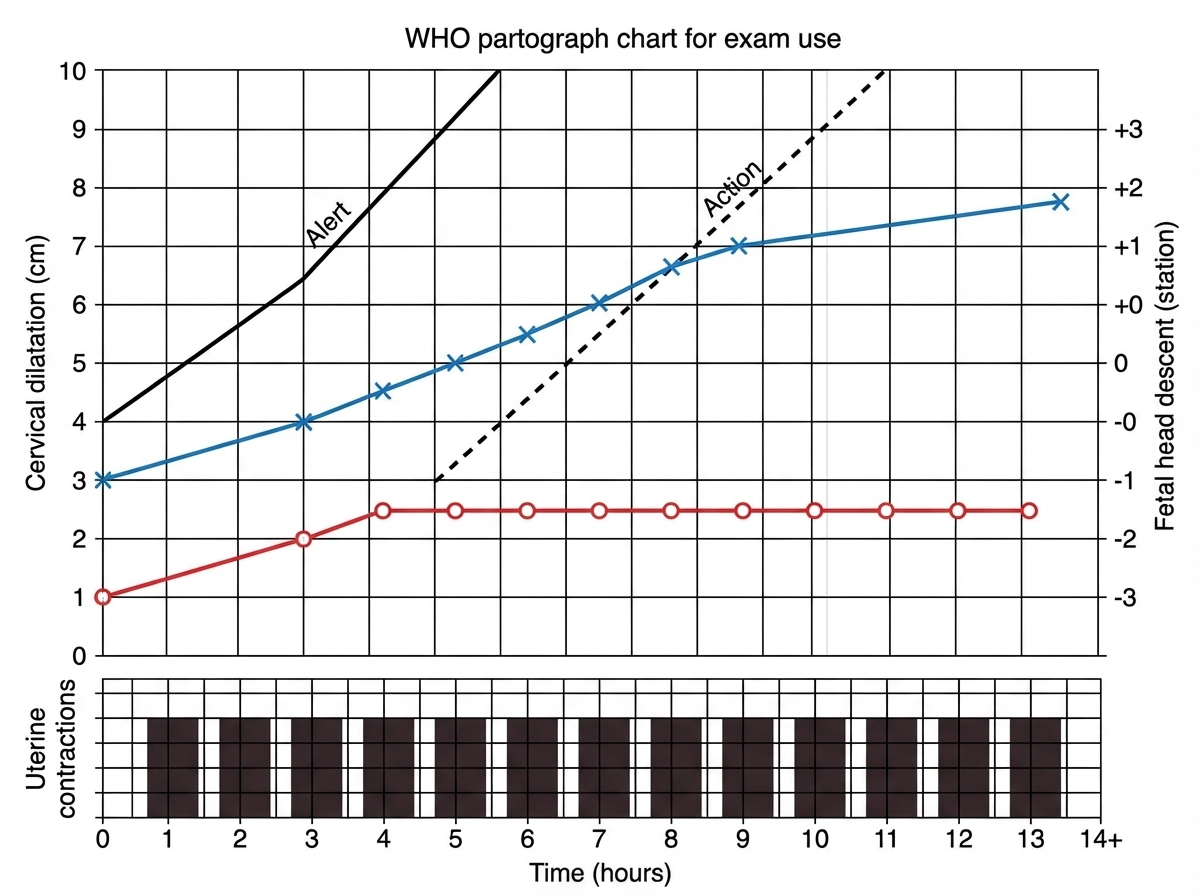
Interpret the given partogram:
A pregnant patient presents with abdominal pain and bleeding per vaginam with a twin gestation of 34 weeks. What is the most probable diagnosis?
What is the best method for induction of labor in cases of hydramnios?
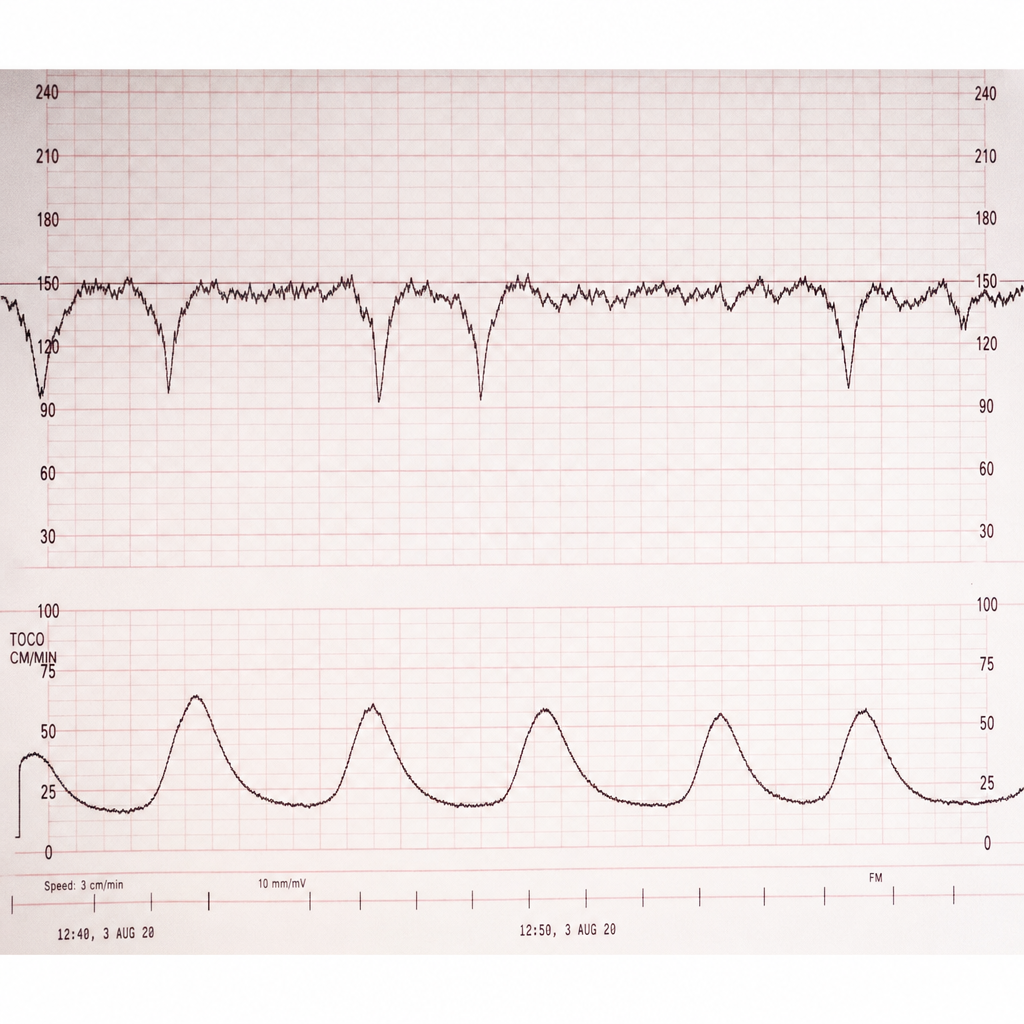
A 30-year-old female patient in labor has the following fetal tocographic finding. What does it suggest?
What is the most common breech presentation in a nulliparous woman?
During delivery, the baby's head was delivered but the shoulders were not delivered after one minute. What is the next step?
A 26-year-old G2P1 woman at 41 weeks gestation has been pushing for 3 hours without progress. Her vaginal examination shows complete dilation, complete effacement, and 0 station, with the fetal head persistently in the occiput posterior position. Which of the following statements accurately describes the situation?
Practice by Chapter
Physiology of Labor
Practice Questions
Stages of Labor and Normal Progression
Practice Questions
Fetal Monitoring Techniques
Practice Questions
Pain Management in Labor
Practice Questions
Induction and Augmentation of Labor
Practice Questions
Operative Delivery (Forceps and Vacuum)
Practice Questions
Cesarean Section: Indications and Techniques
Practice Questions
Dystocia and Abnormal Labor Patterns
Practice Questions
Obstetric Emergencies
Practice Questions
Postpartum Hemorrhage Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app