
Labor and Delivery — MCQs

On this page
In the Bishop score, which of the following components is NOT included?
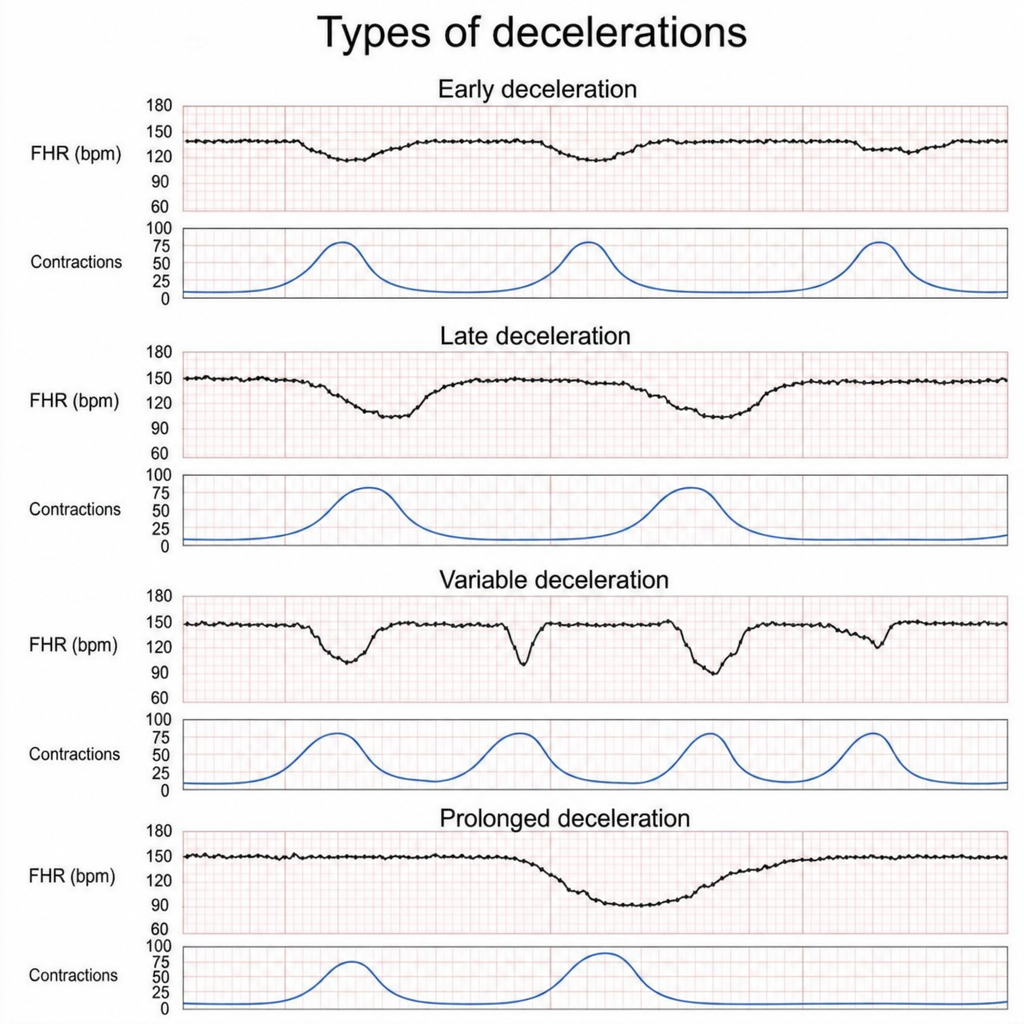
Which of the following is the most probable cause for the deceleration shown below?
Which of the following is a sign of placental separation in stage III of labor?
The usual site of spontaneous rupture of the intact uterus during pregnancy is the:
A 32-week pregnant female with preterm contractions was treated with tocolytic agents. She further developed pulmonary edema. Which of the following tocolytic agents is most likely to have caused pulmonary edema in this patient?
Which of the following is true regarding a fetus in transverse presentation?
Shoulder dystocia is predominantly seen in which of the following conditions?
What percentage of occipitoposterior positions spontaneously convert to the occipitoanterior position and deliver comfortably?
In complete breech presentation, what is the typical fetal attitude maintained?
Which of the following correctly defines Montevideo units for measurement of uterine activity?
Practice by Chapter
Physiology of Labor
Practice Questions
Stages of Labor and Normal Progression
Practice Questions
Fetal Monitoring Techniques
Practice Questions
Pain Management in Labor
Practice Questions
Induction and Augmentation of Labor
Practice Questions
Operative Delivery (Forceps and Vacuum)
Practice Questions
Cesarean Section: Indications and Techniques
Practice Questions
Dystocia and Abnormal Labor Patterns
Practice Questions
Obstetric Emergencies
Practice Questions
Postpartum Hemorrhage Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app