
Labor and Delivery — MCQs

On this page
What is the most common type of female pelvis?
Pelvic outlet is considered contracted if which of the following is true?
Active management of the third stage of labor is most helpful in the prevention of which of the following?
A constriction ring in the uterus is typically seen in which of the following conditions?
In breech presentation, engagement occurs earliest in which type?
Which of the following is true regarding postpartum hemorrhage (PPH)?
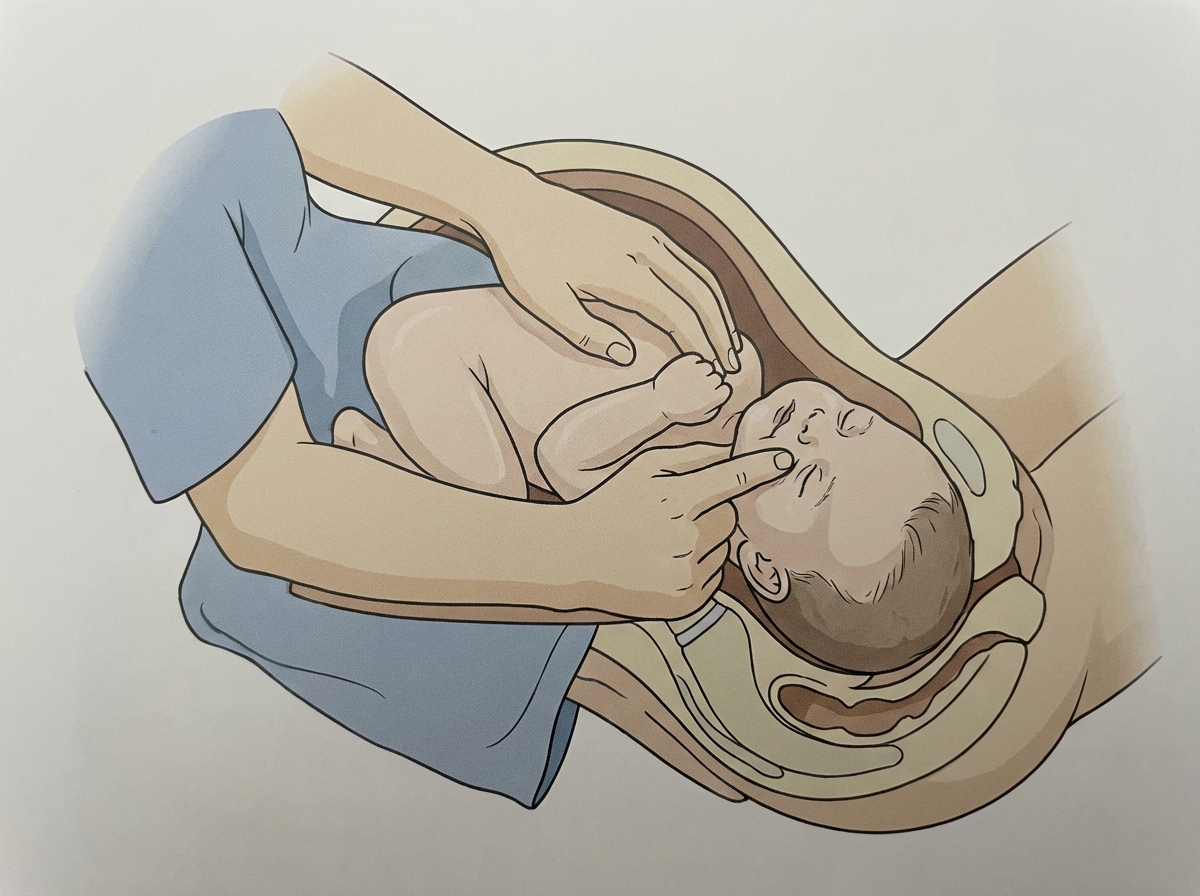
What is the name of the following manoeuvre?
What is the shortest diameter of the pelvic outlet?
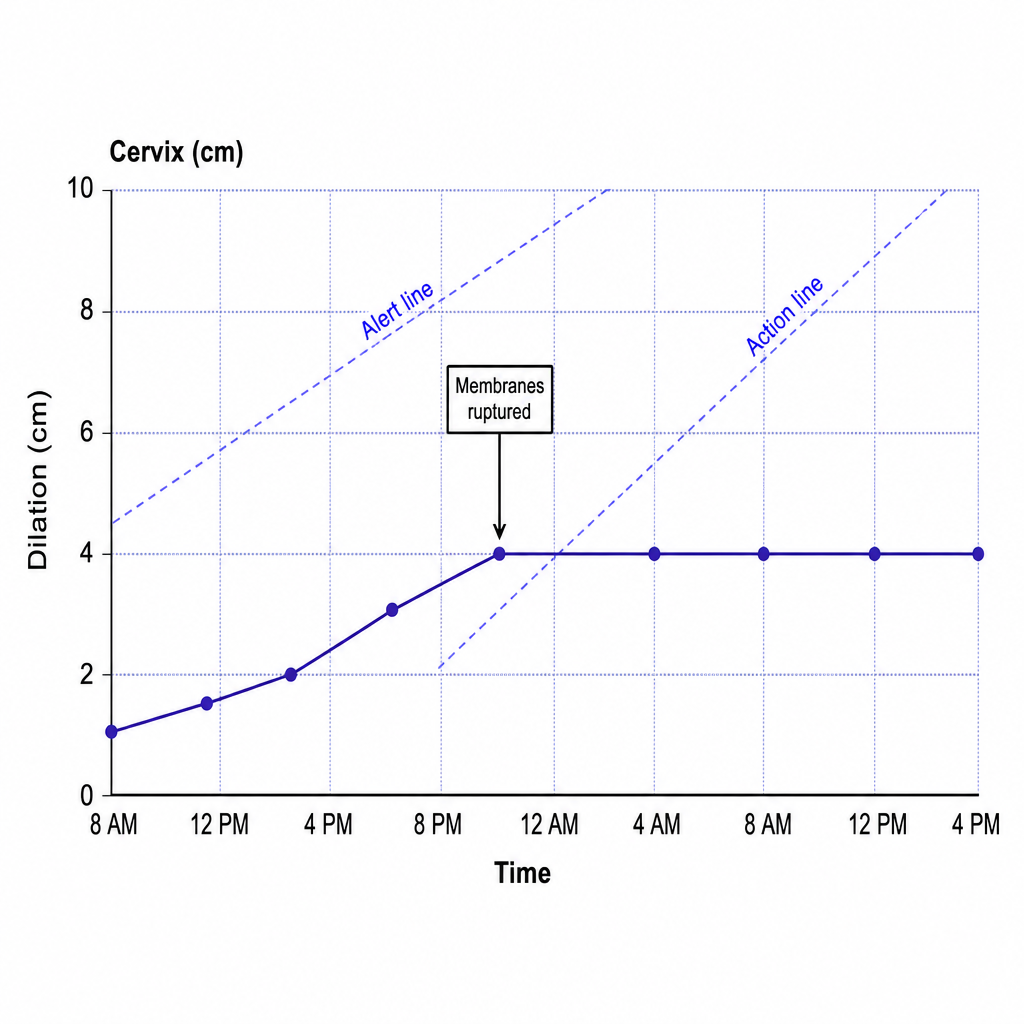
A labor curve for a woman, gravida 3, para 2, at 39 weeks' gestation is shown below. Membranes were ruptured at 6 cm, and she has had adequate uterine contractions for 4 hours without further cervical change. The amniotic fluid was clear, and there has been no indication of fetal distress. Previous infants weighed 3500 g and 3750 g. The estimated weight of this infant, which appears normal on ultrasound, is 3200 g. This labor curve is compatible with which of the following conditions?
All of the following can be administered in acute hypertension during labor except?
Practice by Chapter
Physiology of Labor
Practice Questions
Stages of Labor and Normal Progression
Practice Questions
Fetal Monitoring Techniques
Practice Questions
Pain Management in Labor
Practice Questions
Induction and Augmentation of Labor
Practice Questions
Operative Delivery (Forceps and Vacuum)
Practice Questions
Cesarean Section: Indications and Techniques
Practice Questions
Dystocia and Abnormal Labor Patterns
Practice Questions
Obstetric Emergencies
Practice Questions
Postpartum Hemorrhage Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app