
Labor and Delivery — MCQs

On this page
A woman delivers a 9lb infant and suffers a third-degree tear following a midline episiotomy. Inspection shows which of the following structures is intact?
What is the smallest anteroposterior diameter of the pelvic inlet called?
What is the approximate amount of blood loss when a clot is of fist size?
Which of the following statements is false regarding the cardinal movements during breech delivery?
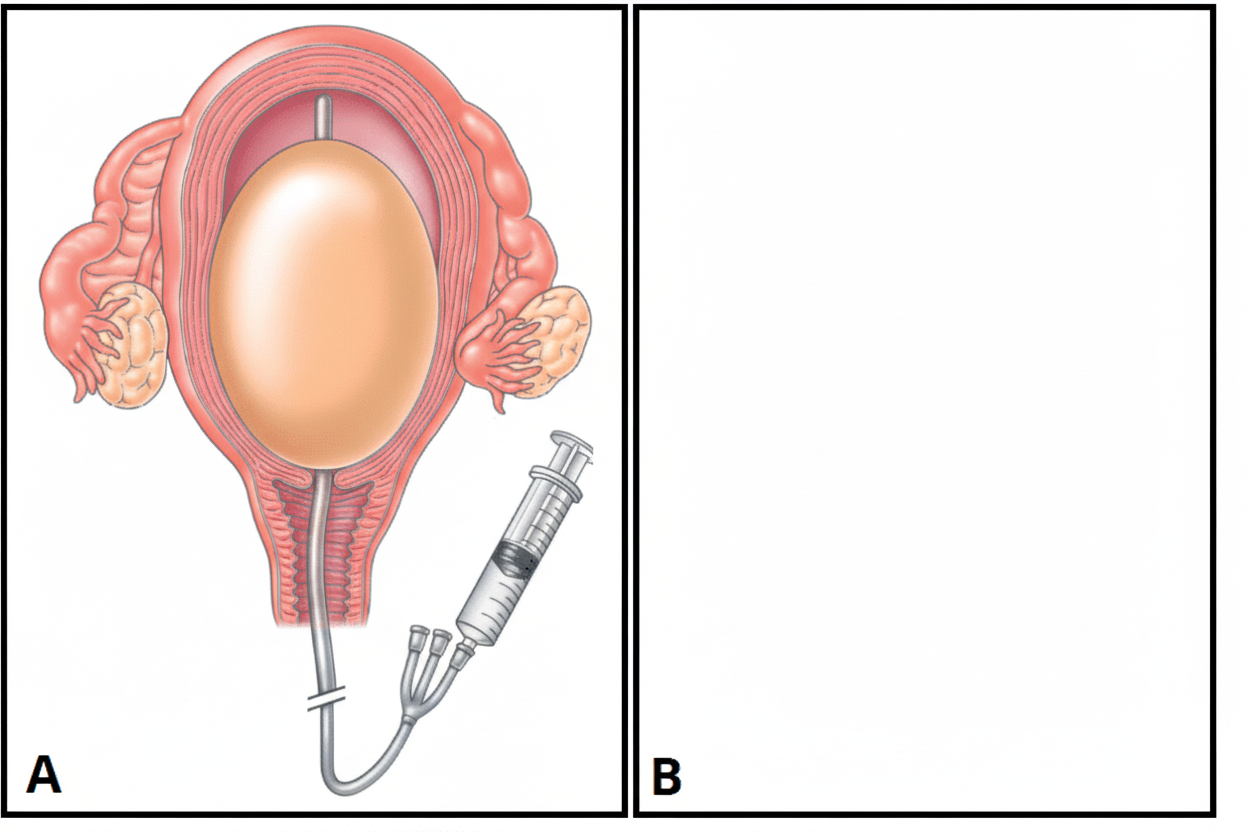
The provided diagram depicts which of the following?
A woman with a previous Lower segment cesarean section will require an elective repeat cesarean section in all of the following conditions, EXCEPT?
On which of the following structures is the B Lynch brace suture applied?
'Flying foetus' is associated with which type of fetal presentation?
Vaginal delivery is not possible in which of the following fetal positions?
What is an indication for the induction of labor?
Practice by Chapter
Physiology of Labor
Practice Questions
Stages of Labor and Normal Progression
Practice Questions
Fetal Monitoring Techniques
Practice Questions
Pain Management in Labor
Practice Questions
Induction and Augmentation of Labor
Practice Questions
Operative Delivery (Forceps and Vacuum)
Practice Questions
Cesarean Section: Indications and Techniques
Practice Questions
Dystocia and Abnormal Labor Patterns
Practice Questions
Obstetric Emergencies
Practice Questions
Postpartum Hemorrhage Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app