
Labor and Delivery — MCQs

On this page
Transverse lie is caused by all except which of the following?
Most common breech presentation in primigravida is?
Persistent OP position is most common in which pelvis?
Which of the following is NOT a contraindication for induction of labour?
Which is the engaging diameter in occipitoposterior presentation?
A multigravida patient with a 4 kg fetus has been in labor for 15 hours, with cervical dilation at 5 cm for the last 8 hours. What is the most appropriate management for this patient?
What is the most common position of engagement in vertex presentation?
Which type of pelvis is most accommodating for the occipitoposterior position during labor?
Which of the following is not typically given to a patient with preterm labor?
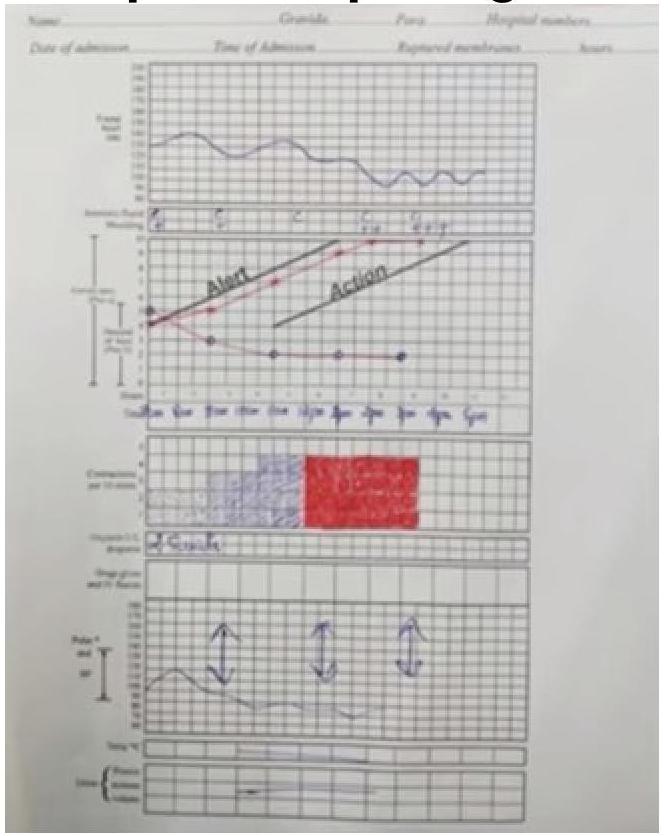
Given the following partogram data, identify the most likely diagnosis: Cervical dilation curve shows a prolonged labor with the cervical dilation falling to the right of the alert line.
Practice by Chapter
Physiology of Labor
Practice Questions
Stages of Labor and Normal Progression
Practice Questions
Fetal Monitoring Techniques
Practice Questions
Pain Management in Labor
Practice Questions
Induction and Augmentation of Labor
Practice Questions
Operative Delivery (Forceps and Vacuum)
Practice Questions
Cesarean Section: Indications and Techniques
Practice Questions
Dystocia and Abnormal Labor Patterns
Practice Questions
Obstetric Emergencies
Practice Questions
Postpartum Hemorrhage Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app