
Labor and Delivery — MCQs

On this page
Which of the following measures does NOT help prevent perineal injury during normal labor?
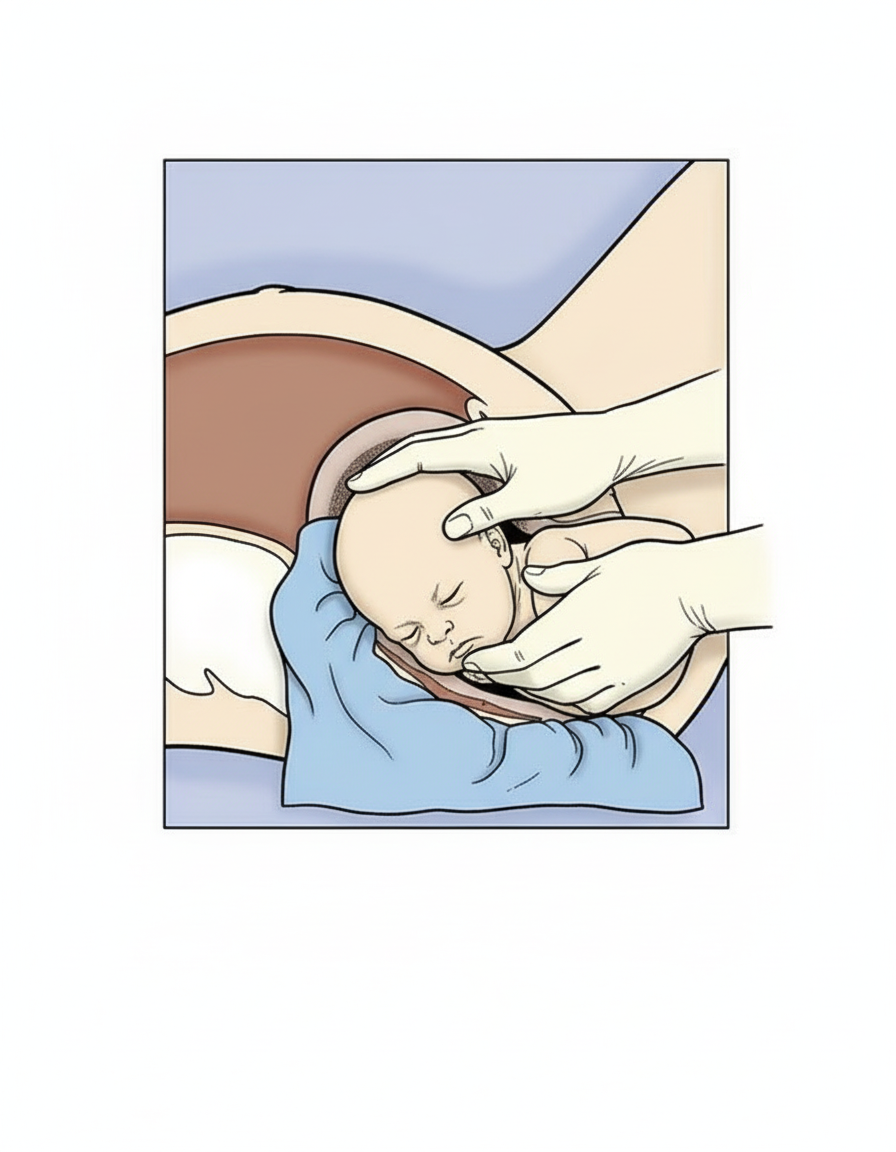
Which maneuver is being shown below?
Variable deceleration indicates:
Which of the following is NOT a cause of prolonged first stage of labor?
A 16-year-old female presents with severe abdominal pain and fever. Laboratory findings include an elevated white blood cell count and a positive pregnancy test. Colpocentesis is performed to identify pelvic blood, potentially from a ruptured ectopic pregnancy. Through which of the following structures is the needle inserted?
The distance from the upper end of sacrum to the lower border of the pubis corresponds to which conjugate?
What is the largest transverse diameter of the fetal head?
Recurrent breech presentation is due to:
A 25-year-old G2P2 patient with B negative blood group presents in active labor and is fully dilated. Which of the following standard procedures should NOT be followed in this patient?
Which drug is NOT used in the management of postpartum hemorrhage (PPH)?
Practice by Chapter
Physiology of Labor
Practice Questions
Stages of Labor and Normal Progression
Practice Questions
Fetal Monitoring Techniques
Practice Questions
Pain Management in Labor
Practice Questions
Induction and Augmentation of Labor
Practice Questions
Operative Delivery (Forceps and Vacuum)
Practice Questions
Cesarean Section: Indications and Techniques
Practice Questions
Dystocia and Abnormal Labor Patterns
Practice Questions
Obstetric Emergencies
Practice Questions
Postpartum Hemorrhage Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app