
Gynecological Disorders — MCQs

On this page
What is the commonest site for a fibroid?
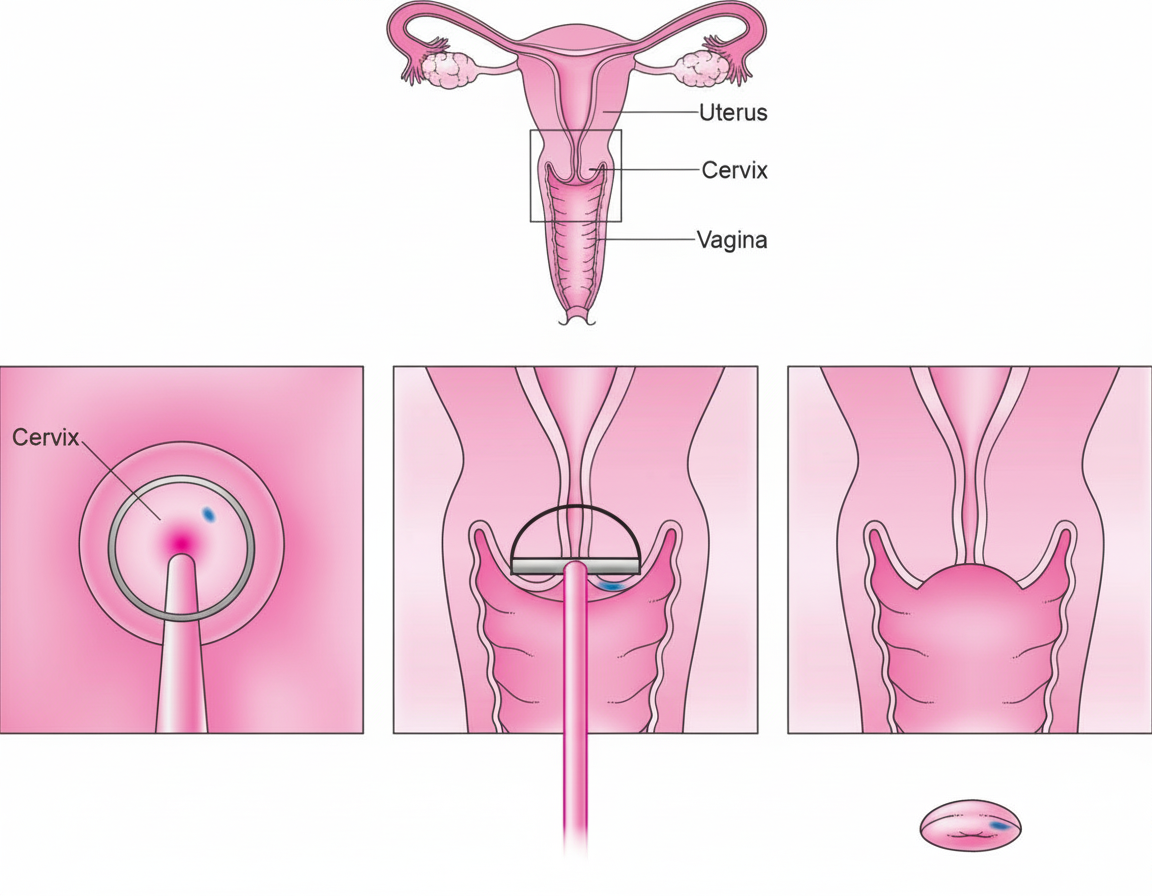
The procedure shown below is
A 28-week pregnant patient presents with abdominal pain and fever. Ultrasonography reveals the presence of a fibroid. What is the next line of management?
Fothergill's repair is also known as:
During pregnancy, fibroid may have all of the following complications except:
What is the primary treatment for endometriosis in a younger age group?
Which of the following findings is suggestive of a Bicornuate uterus?
Which of the following is the most widely accepted theory explaining the development of endometriosis?
Which of the following is NOT a risk factor for acute pelvic inflammatory disease (PID)?
All of the following are included in Amsler's criteria, EXCEPT:
Practice by Chapter
Abnormal Uterine Bleeding
Practice Questions
Endometriosis
Practice Questions
Adenomyosis
Practice Questions
Uterine Fibroids
Practice Questions
Ovarian Cysts
Practice Questions
Pelvic Inflammatory Disease
Practice Questions
Vulvovaginitis
Practice Questions
Pelvic Organ Prolapse
Practice Questions
Vulvar Disorders
Practice Questions
Benign Breast Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app