
Gynecological Disorders — MCQs

On this page
Which of the following does NOT predispose to isoimmunization in an Rh-negative female?
What is the mechanism responsible for high rates of spontaneous abortion in a septate uterus?
What is the best investigation to establish the diagnosis of endometriosis?
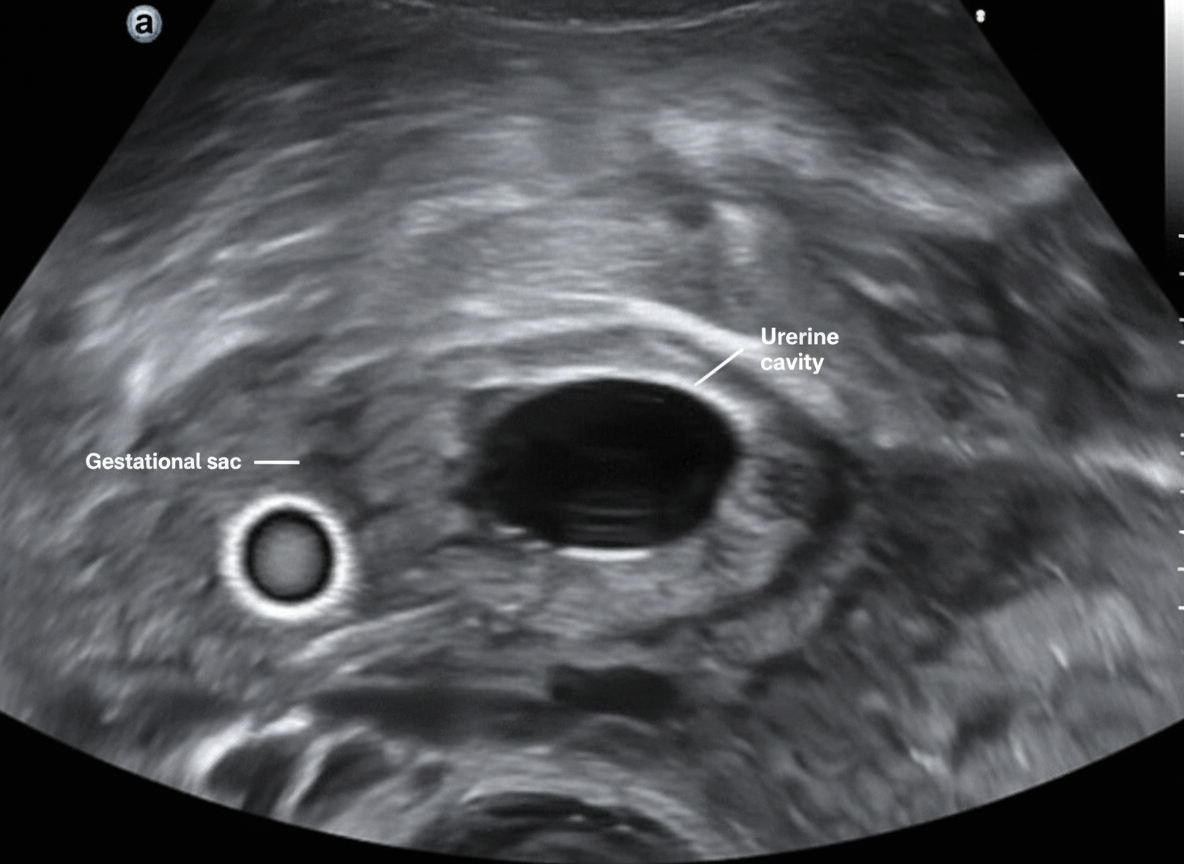
What is pathognomonic of ectopic pregnancy?
Which of the following conditions is NOT associated with the pathology shown in the ultrasound image?
Which of the following is NOT a complication of hysterectomy?
A 45-year-old postmenopausal woman presents with vaginal bleeding. Transvaginal ultrasound reveals an endometrial thickness of 8.0 mm. What is the next step in management?
Hematocolpos is seen in which of the following conditions?
What is the sensitivity of a conventional Pap smear in detecting cervical cancer?
Curdy vaginal discharge is characteristic of which infection?
Practice by Chapter
Abnormal Uterine Bleeding
Practice Questions
Endometriosis
Practice Questions
Adenomyosis
Practice Questions
Uterine Fibroids
Practice Questions
Ovarian Cysts
Practice Questions
Pelvic Inflammatory Disease
Practice Questions
Vulvovaginitis
Practice Questions
Pelvic Organ Prolapse
Practice Questions
Vulvar Disorders
Practice Questions
Benign Breast Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app