
Gynecological Disorders — MCQs

On this page
60-year-old female with a history of intermittent bleeding. Saline infusion sonography reveals a well-defined, smooth-bordered intracavitary mass with a single feeding vessel on Doppler at its base. What is the most likely diagnosis based on these findings?

A mother brought her 16-year-old daughter to Gynaecology OPD with a complaint of not attending menarche. She gives a history of cyclic abdominal pain. On further examination, a midline abdominal swelling is seen. Per rectal examination reveals a bulging mass in the vaginal area. Which of the following can be most commonly seen?
Long-standing pelvic inflammatory disease (PID) may lead to which of the following complications?
What type of uterine anomaly is shown in this X-ray HSG image?

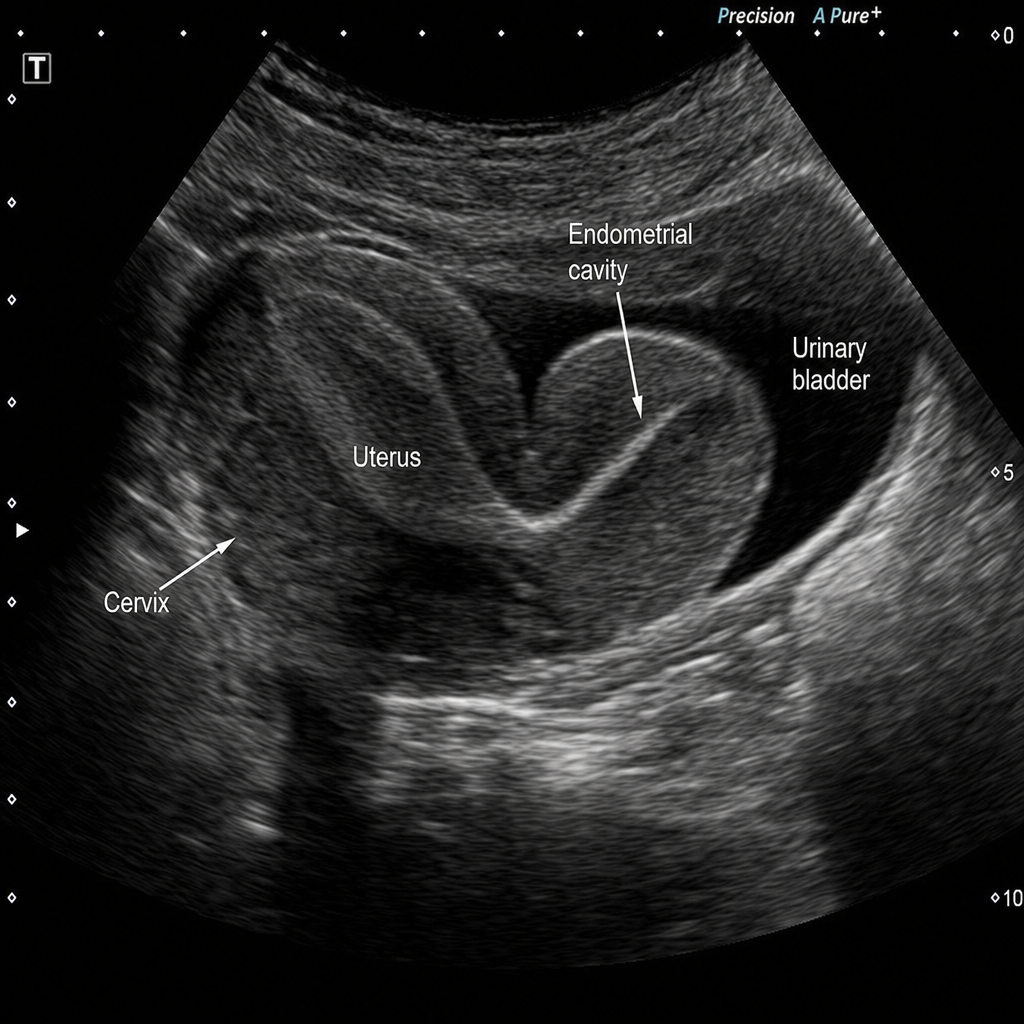
This sagittal pelvic ultrasound image is being reviewed for a possible Müllerian uterine anomaly. Which interpretation is most appropriate?
Dilatation & curettage (D&C) is contraindicated in-
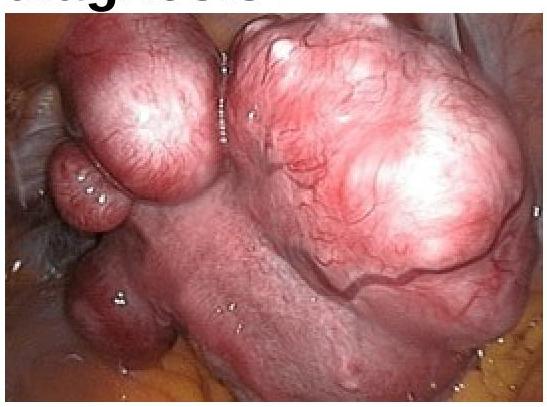
In a woman complaining of AUB following image was seen in laparoscopic examination of uterus. What will be the diagnosis?
What is the most common cause of pelvic inflammatory disease?
Which of the following conditions is most commonly associated with malodorous vaginal discharge?
In which part of the fallopian tube is ectopic pregnancy most likely to survive longer?
Practice by Chapter
Abnormal Uterine Bleeding
Practice Questions
Endometriosis
Practice Questions
Adenomyosis
Practice Questions
Uterine Fibroids
Practice Questions
Ovarian Cysts
Practice Questions
Pelvic Inflammatory Disease
Practice Questions
Vulvovaginitis
Practice Questions
Pelvic Organ Prolapse
Practice Questions
Vulvar Disorders
Practice Questions
Benign Breast Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app