
Gynecological Disorders — MCQs

On this page
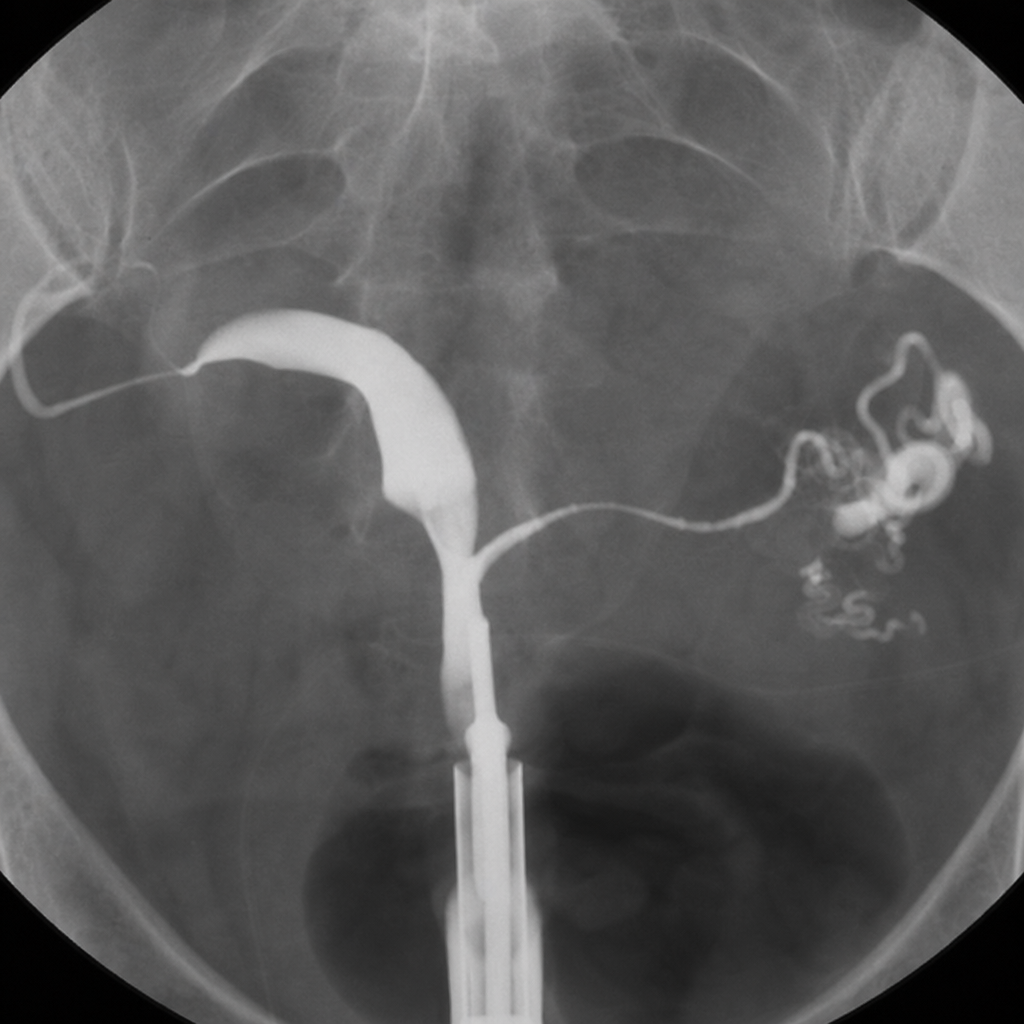
Identify the X-ray HSG image shown below:
Which of the following is NOT a risk factor for ectopic pregnancy?
What is the primary mechanism proposed by Sampson's theory for the development of endometriosis?
Which of the following is NOT part of the classic triad of symptoms associated with endometriosis?
What is the most common cause for hysterectomy?
What is the most common presenting symptom of fibroids?
Which of the following best describes endometriosis?
Kamla, a 30-year-old woman, P2L2 with a 3.2 x 4.1 cm fibroid uterus, presents with menorrhagia and has been on symptomatic treatment for the past 6 months. She refuses surgery. What is the next line of management?
What is the definitive treatment for adenomyosis?
What is the surgery of choice for a 42-year-old woman with diffuse endometriosis?
Practice by Chapter
Abnormal Uterine Bleeding
Practice Questions
Endometriosis
Practice Questions
Adenomyosis
Practice Questions
Uterine Fibroids
Practice Questions
Ovarian Cysts
Practice Questions
Pelvic Inflammatory Disease
Practice Questions
Vulvovaginitis
Practice Questions
Pelvic Organ Prolapse
Practice Questions
Vulvar Disorders
Practice Questions
Benign Breast Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app