
Gynecological Disorders — MCQs

On this page
A 32-year-old woman presents with menorrhagia and dysmenorrhea. An ultrasound reveals adenomyosis. What is the best initial treatment option for this condition?
A 30-year-old woman presents with abnormal uterine bleeding and an enlarged uterus. Which diagnostic test is the most appropriate?
What non-surgical intervention is primarily used to manage patients with symptomatic uterine fibroids who wish to retain their fertility?
A 28-year-old woman is diagnosed with gonococcal cervicitis (NAAT positive for Neisseria gonorrhoeae) and presents with purulent cervical discharge. What is the most likely complication if left untreated?
A 30-year-old woman presents with secondary amenorrhea and a history of curettage. What is the diagnosis?
A 30-year-old woman presents with vaginal discharge and pelvic pain. Examination reveals cervical motion tenderness. What is the next step?
A 34-year-old woman presents with pelvic pain and a palpable adnexal mass. The CA-125 level is elevated. What is the next best step in management?
60 yr female with a history of intermittent bleeding. What is the diagnosis based on the ultrasound image?
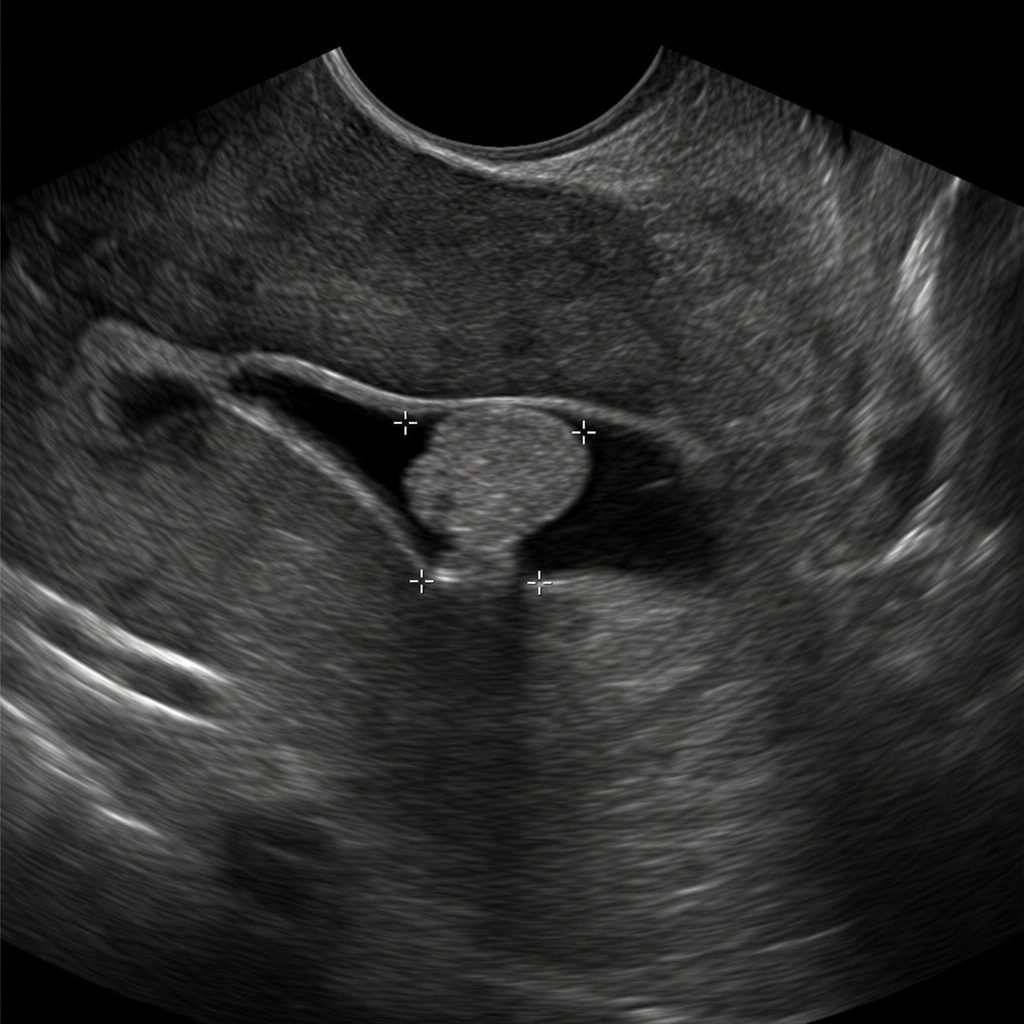
Based on the provided image, which of the following is the correct diagnosis?

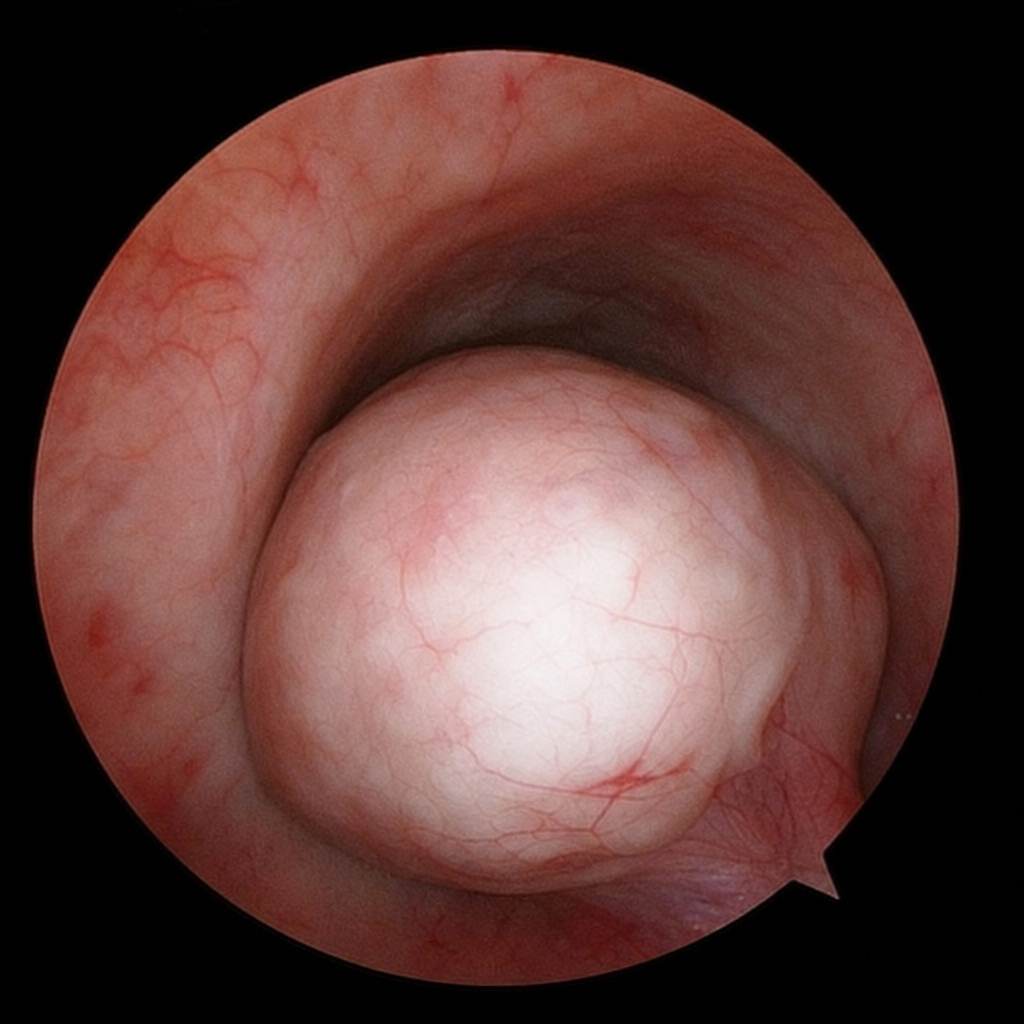
In a woman complaining of AUB, the following image was seen in endoscopic examination of uterus. What will be the diagnosis?
Practice by Chapter
Abnormal Uterine Bleeding
Practice Questions
Endometriosis
Practice Questions
Adenomyosis
Practice Questions
Uterine Fibroids
Practice Questions
Ovarian Cysts
Practice Questions
Pelvic Inflammatory Disease
Practice Questions
Vulvovaginitis
Practice Questions
Pelvic Organ Prolapse
Practice Questions
Vulvar Disorders
Practice Questions
Benign Breast Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app