
Gynecological Disorders — MCQs

On this page
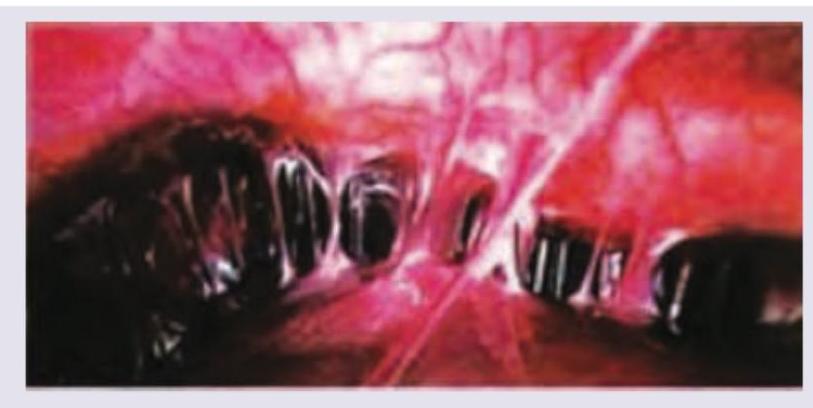
Which one of the following is implicated in the etiology of these adhesions around the liver?
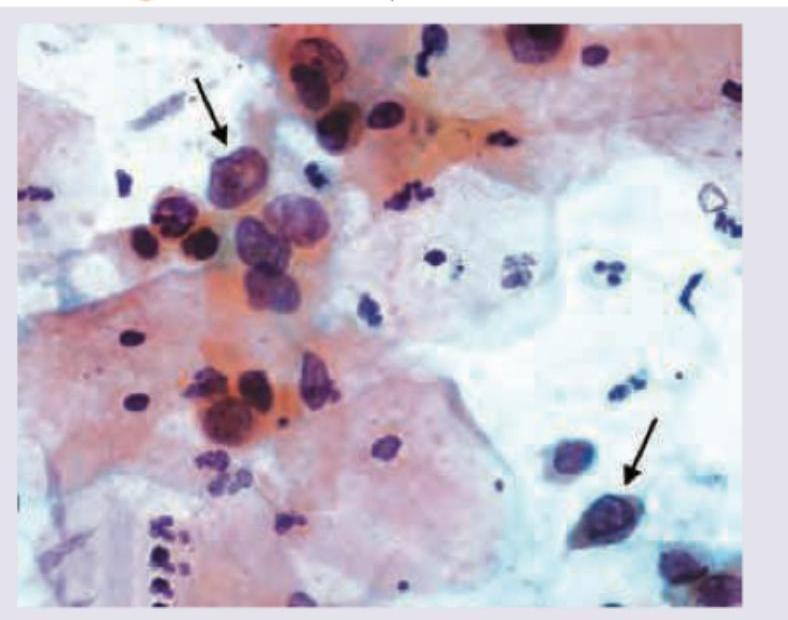
Which characteristic cell is shown in the Pap smear taken in a 31-year-old woman with normal menses taken in pre-ovulatory stage? She complains of occasional postcoital bleeding.
A 28 -year-old P_2 ~L_2 presents to Gynaecology OPD with complaints of malodorous vaginal discharge. On examination, the discharge was found to be grayish-white in colour and adherent to vaginal walls. Which one of the following is a bedside diagnostic criterion for the causative organism?
Which one of the following is not a differential diagnosis of chronic inversion of uterus?
What are the characteristics of dermoid cyst? I. Germ cell ovarian tumour II. Bilateral in 15-20 % cases III. Torsion is common IV. Rupture is common Select the correct answer using the code given below :
Which of the following are Amsel's diagnostic criteria? I. Vaginal pH>4.5 II. Positive Whiff test III. Presence of clue cells >20 % IV. Positive bacterial vaginal culture Select the correct answer using the code given below :
For which of the following conditions, surgery is indicated in a case of Fibroid Uterus ? I. Symptomatic and failed medical management II. Size >12 weeks III. Pedunculated fibroid Select the correct answer using the code given below :
Which of the following are indications of endometrial sampling? I. Routine screening in asymptomatic premenopausal women II. Endometrial polyp III. Postmenopausal bleeding IV. Abnormal uterine bleeding Select the correct answer using the code given below :
Which one of the following is the distinguishing feature to differentiate Gartner's cyst from Cystocele ?
Which of the following are symptoms of genital tuberculosis? 1. Postmenopausal bleeding 2. Infertility 3. Chronic pelvic pain 4. Oligomenorrhoea Select the correct answer using the code given below.
Practice by Chapter
Abnormal Uterine Bleeding
Practice Questions
Endometriosis
Practice Questions
Adenomyosis
Practice Questions
Uterine Fibroids
Practice Questions
Ovarian Cysts
Practice Questions
Pelvic Inflammatory Disease
Practice Questions
Vulvovaginitis
Practice Questions
Pelvic Organ Prolapse
Practice Questions
Vulvar Disorders
Practice Questions
Benign Breast Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app