
Gynecological Disorders — MCQs

On this page
What is shown below in the image of a PID patient?

A 28 -year-old female patient presented with lower abdominal pain along with dysmenorrhea. The following finding was seen on laparoscopic examination. What is the likely diagnosis?

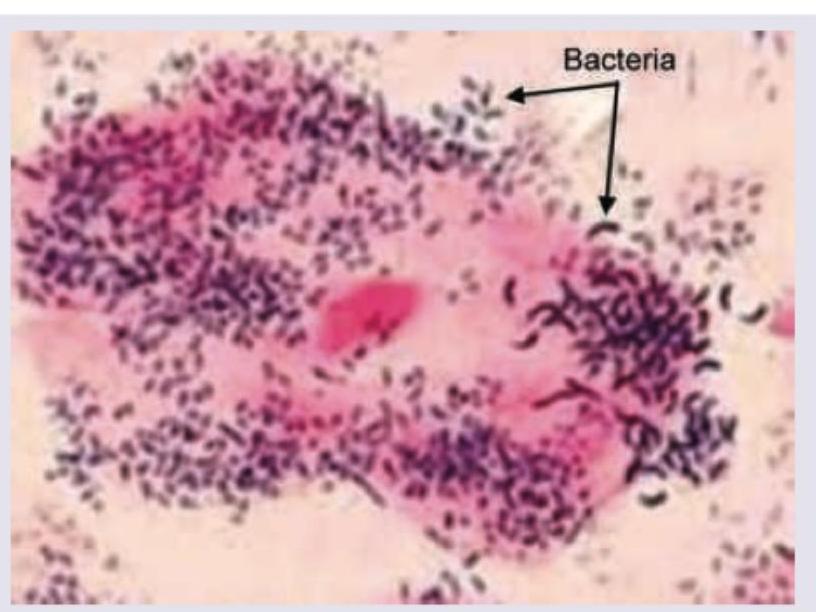
A 21-year-old girl is having vaginal discharge. The smear of vaginal discharge is shown below. BV is not classified as an STI. All are Amsel criteria for the condition shown except:
Which of the following is used in the gynecological procedure being performed in the image?
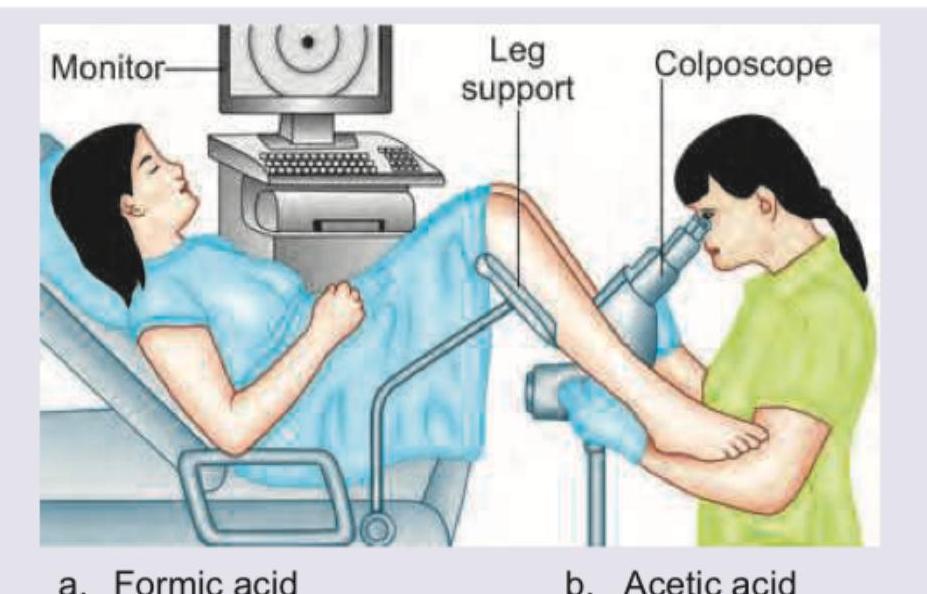
The procedure being performed is called:
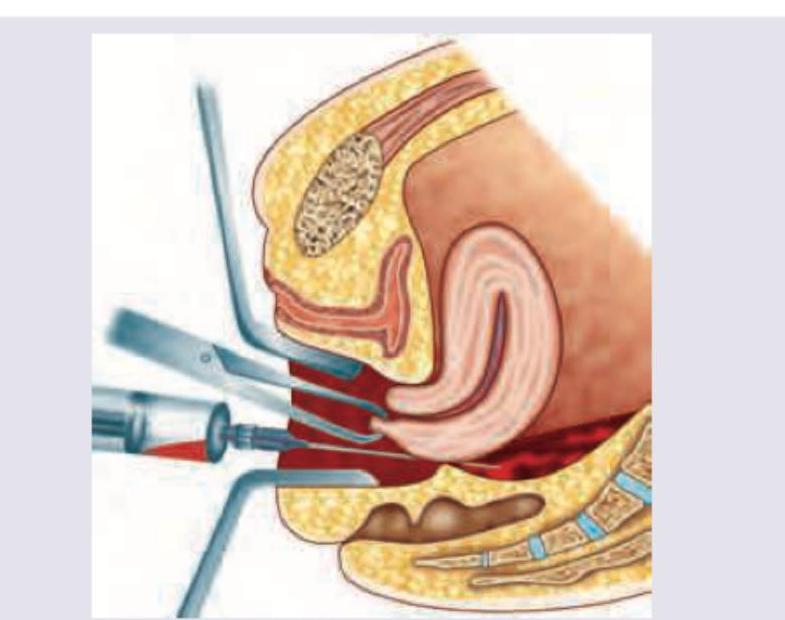
The image shows: (Recent Neet Pattern 2016-17)
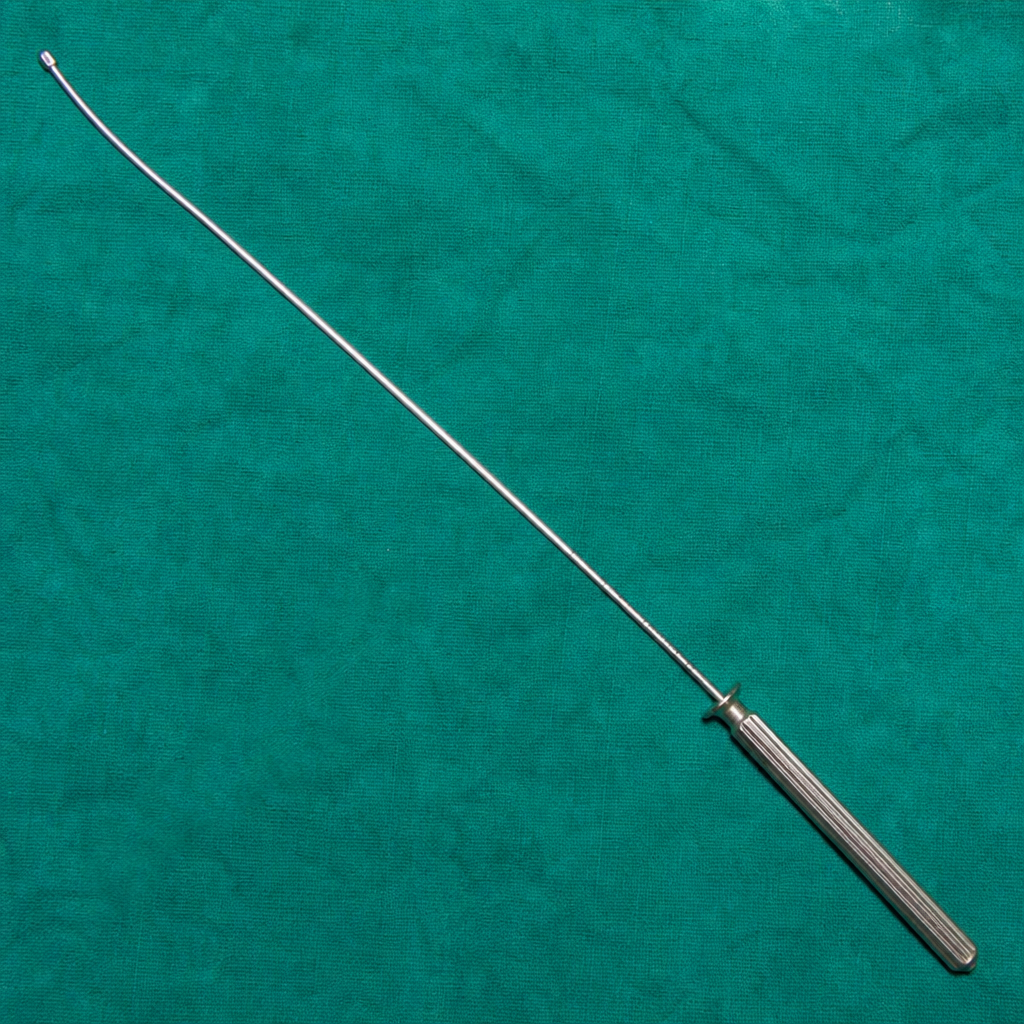
The image shows: (Recent Neet Pattern 2016-17)

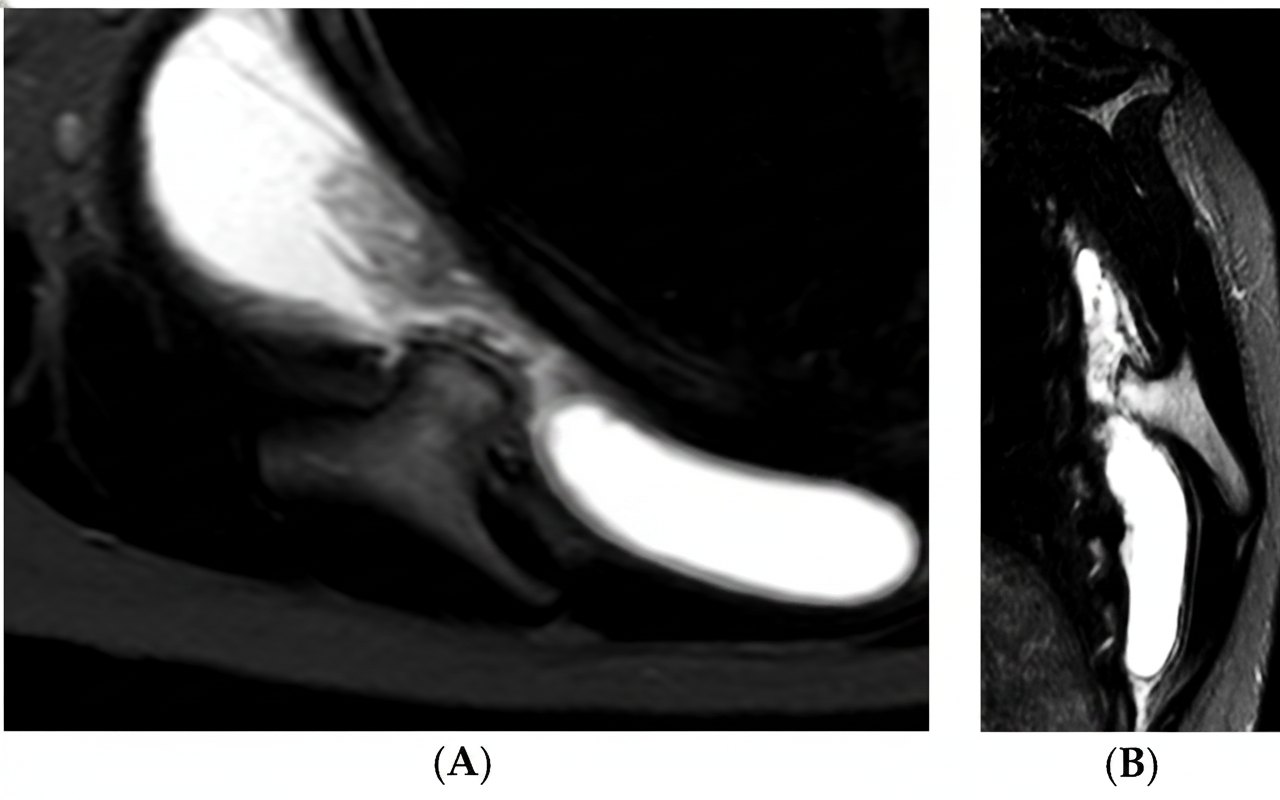
A patient undergoes pelvic MRI, which demonstrates a fluid-filled cyst along the anterolateral vaginal wall. What is the most likely diagnosis?
What is the best treatment for the condition shown below?
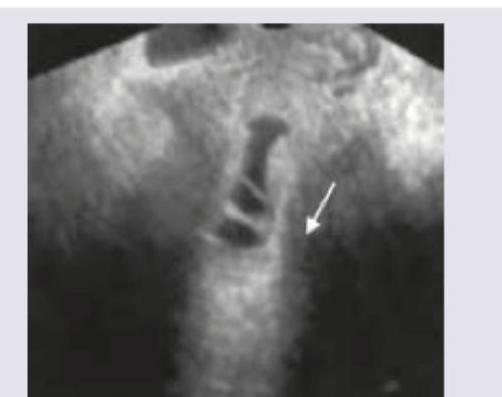
Transvaginal saline infusion sonographic evaluation shows:

Practice by Chapter
Abnormal Uterine Bleeding
Practice Questions
Endometriosis
Practice Questions
Adenomyosis
Practice Questions
Uterine Fibroids
Practice Questions
Ovarian Cysts
Practice Questions
Pelvic Inflammatory Disease
Practice Questions
Vulvovaginitis
Practice Questions
Pelvic Organ Prolapse
Practice Questions
Vulvar Disorders
Practice Questions
Benign Breast Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app