
Gynecological Disorders — MCQs

On this page
Identify the instrument shown below:
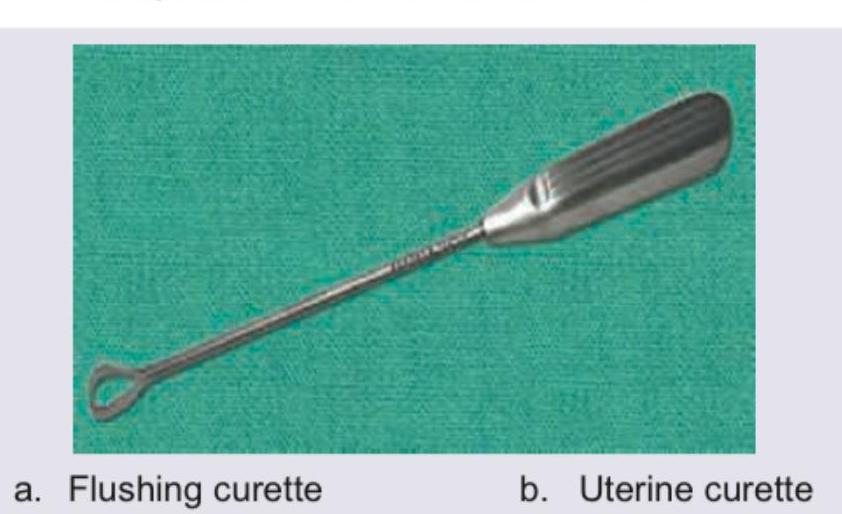
What is incorrect about this instrument?
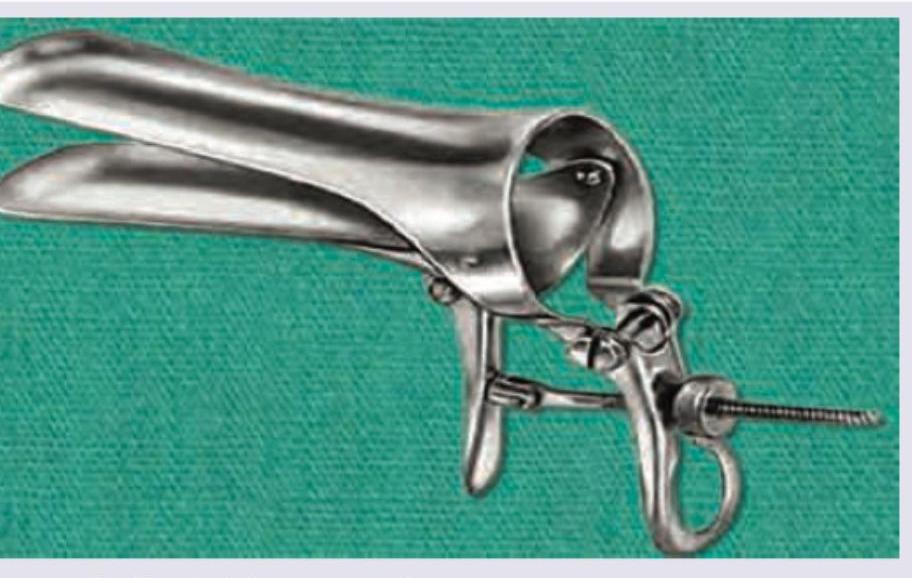
Which of the following is incorrect about the instrument shown below? (Recent Neet Pattern 2016-17)
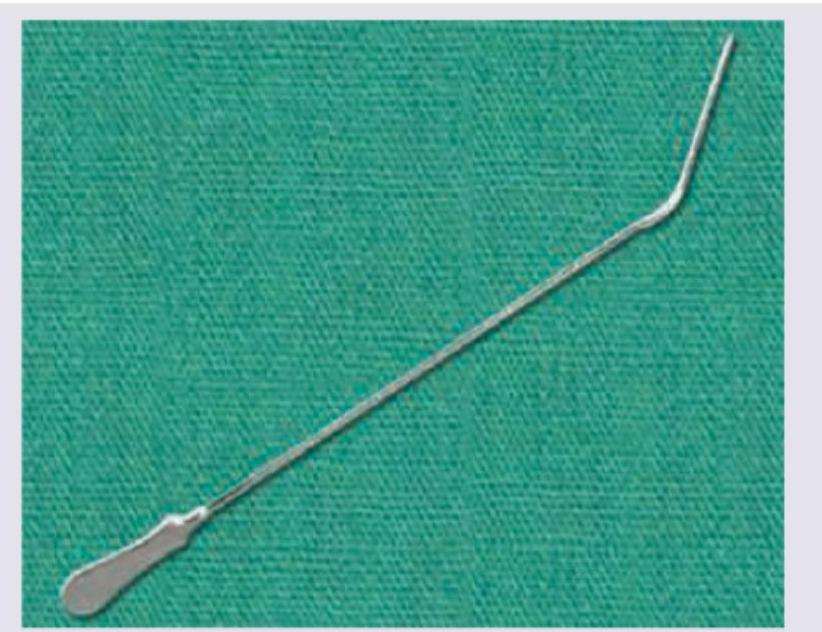
What is the instrument shown below used for?

The following hysteroscopy view shows presence of: (Recent Neet Pattern 2016-17)
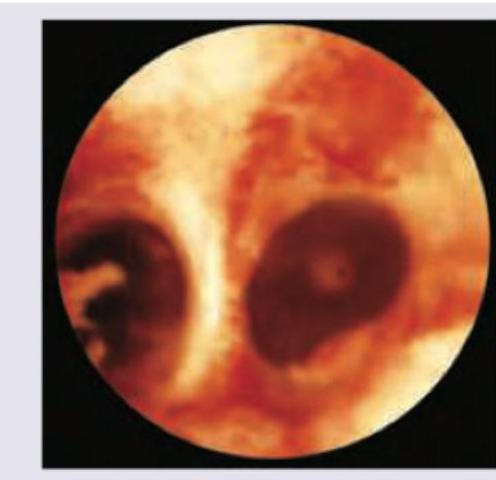
All the following statements regarding the picture are true except: (Recent Neet Pattern 2016-17)

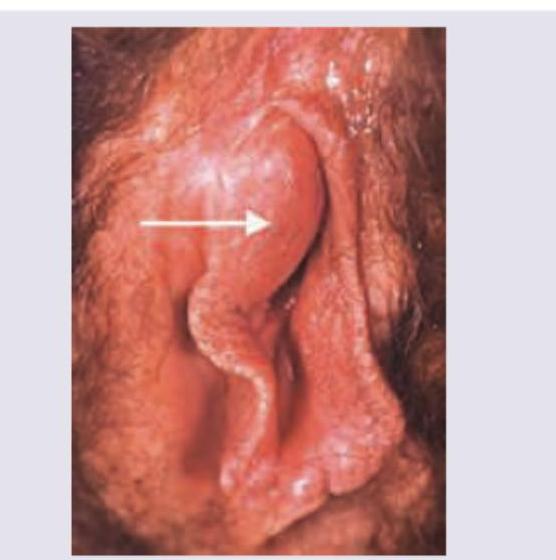
A 23-year-old woman presents to your clinic with complaints of vulvar pain. The patient's history is significant for a new sexual partner and a recent history of flu-like symptoms and vaginal burning. On physical examination, extremely painful shallow ulcers with red borders are appreciated on the vulva, vagina, and perineal region. Which of the following is the most appropriate course of treatment for this patient?
Name the condition shown in the image.
HSG image given below shows:

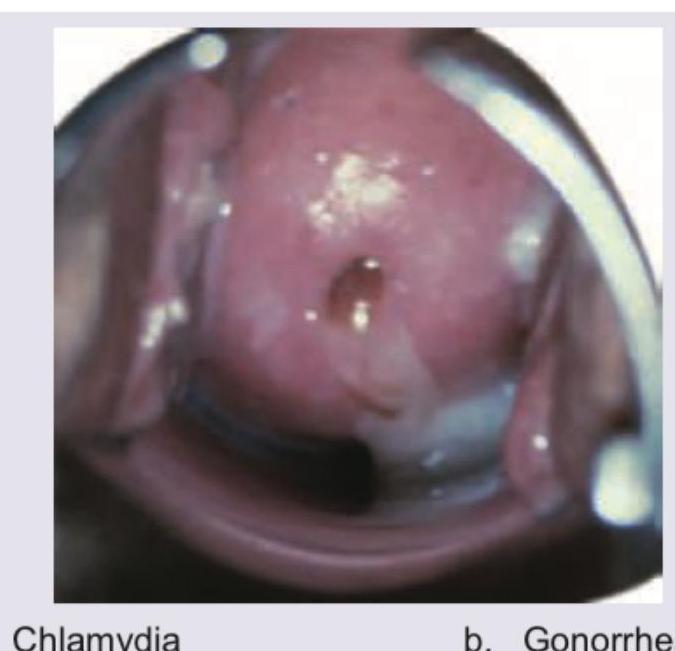
A patient presents with the cervical findings shown. A nucleic acid amplification test (NAAT) returns positive for an obligate intracellular bacterium that targets columnar epithelium and is the most common bacterial STD in the United States. Identify the STD. (Recent Neet Pattern 2016-17)
Practice by Chapter
Abnormal Uterine Bleeding
Practice Questions
Endometriosis
Practice Questions
Adenomyosis
Practice Questions
Uterine Fibroids
Practice Questions
Ovarian Cysts
Practice Questions
Pelvic Inflammatory Disease
Practice Questions
Vulvovaginitis
Practice Questions
Pelvic Organ Prolapse
Practice Questions
Vulvar Disorders
Practice Questions
Benign Breast Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app