
Gynecological Disorders — MCQs

On this page
What is the likely diagnosis for the given image?
A young sexually active female patient presented to the outpatient department with complaints of lower abdominal pain, fever, vomiting, and foul-smelling vaginal discharge. On examination, the body temperature is 103 degrees Fahrenheit, pulse rate is 109 per minute and there is abdominal tenderness. Cervical motion tenderness is present on examination. What is the most likely diagnosis?
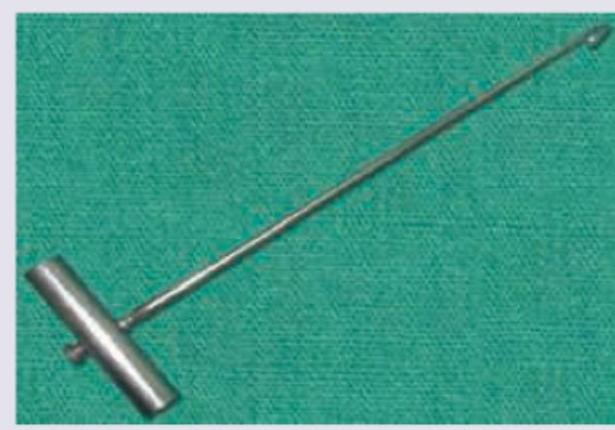
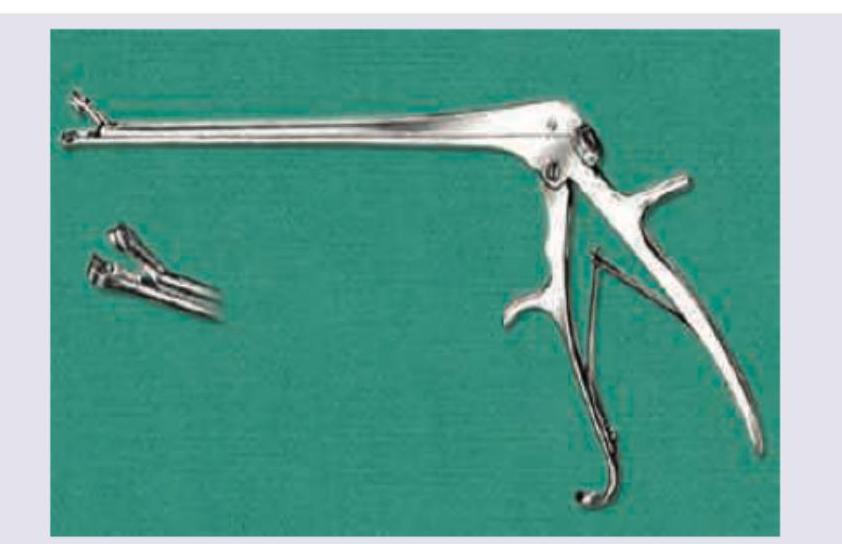
Which of the following procedures is done with the instrument shown below? 
Which of the following procedures is done with the instrument shown below?

A woman presents with complaints of greenish-frothy vaginal discharge for 1 month. On examination, vulvovaginal erythema is noticed. On saline microscopy, motile organisms are seen. What is the most likely diagnosis?
A 26-year-old woman presents with amenorrhea for 8 weeks, lower abdominal pain, and vaginal spotting. Beta-hCG is 3,500 mIU/mL. Transvaginal ultrasound shows an empty uterus with a 3 cm adnexal mass and moderate free fluid in the pouch of Douglas. Vital signs are stable. What is the most appropriate management?
A 42-year-old woman presents with chronic lower abdominal pain and dysmenorrhea. MRI shows diffuse uterine enlargement with junctional zone thickening and scattered high-signal foci in the myometrium. What is the most likely diagnosis?
Identify the instrument shown below:
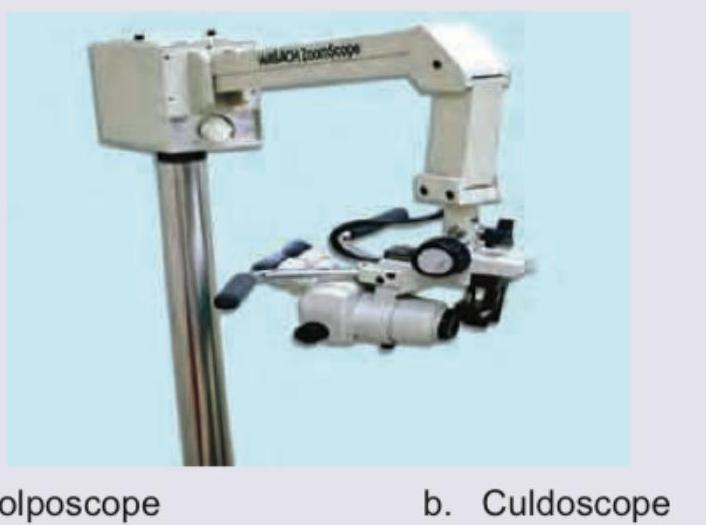
Identify the instrument shown below:
Identify the instrument shown below:
Practice by Chapter
Abnormal Uterine Bleeding
Practice Questions
Endometriosis
Practice Questions
Adenomyosis
Practice Questions
Uterine Fibroids
Practice Questions
Ovarian Cysts
Practice Questions
Pelvic Inflammatory Disease
Practice Questions
Vulvovaginitis
Practice Questions
Pelvic Organ Prolapse
Practice Questions
Vulvar Disorders
Practice Questions
Benign Breast Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app