
Gynecological Disorders — MCQs

On this page
Toxic shock syndrome is due to what?
The squamocolumnar junction lies outside the external os in all of the following conditions EXCEPT:
Which of the following Mullerian duct anomalies is associated with the presence of two cervices?
What uterine anomaly is characterized by a banana-shaped uterus?
Which of the following is NOT true about transverse vaginal septum?
Which of the following is FALSE about bacterial vaginosis?
Retention of urine is a feature in which of the following?
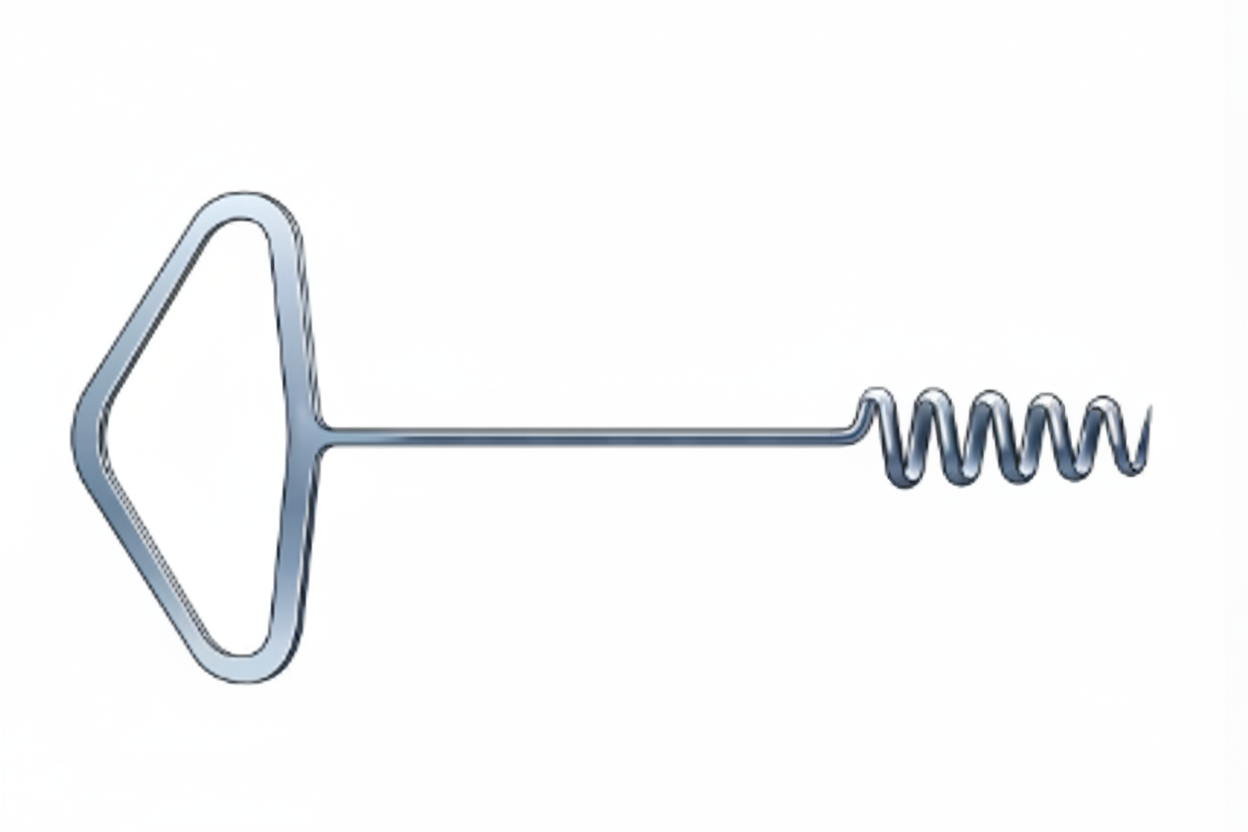
For which procedure is this instrument primarily designed?
A 25-year-old female presents with a two-year history of trying to conceive. Her medical history includes cyclical pelvic pain, dysmenorrhea, dyspareunia, and infertility. Physical examination reveals diffuse abdominal or pelvic pain of variable location, nodular thickening and tenderness along the uterosacral ligaments, on the posterior surface of the uterus, and in the posterior cul-de-sac, scarring and narrowing of the posterior vaginal fornix, and adnexal enlargement and tenderness. What is your diagnosis?
Which of the following is true with regards to genital tuberculosis?
Practice by Chapter
Abnormal Uterine Bleeding
Practice Questions
Endometriosis
Practice Questions
Adenomyosis
Practice Questions
Uterine Fibroids
Practice Questions
Ovarian Cysts
Practice Questions
Pelvic Inflammatory Disease
Practice Questions
Vulvovaginitis
Practice Questions
Pelvic Organ Prolapse
Practice Questions
Vulvar Disorders
Practice Questions
Benign Breast Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app