
Gynecological Disorders — MCQs

On this page
Which of the following fluids or gases are used for hysteroscopy?
What is the distention medium typically used in diagnostic hysteroscopy with bipolar energy?
What is the commonest degenerative change observed in uterine myoma?
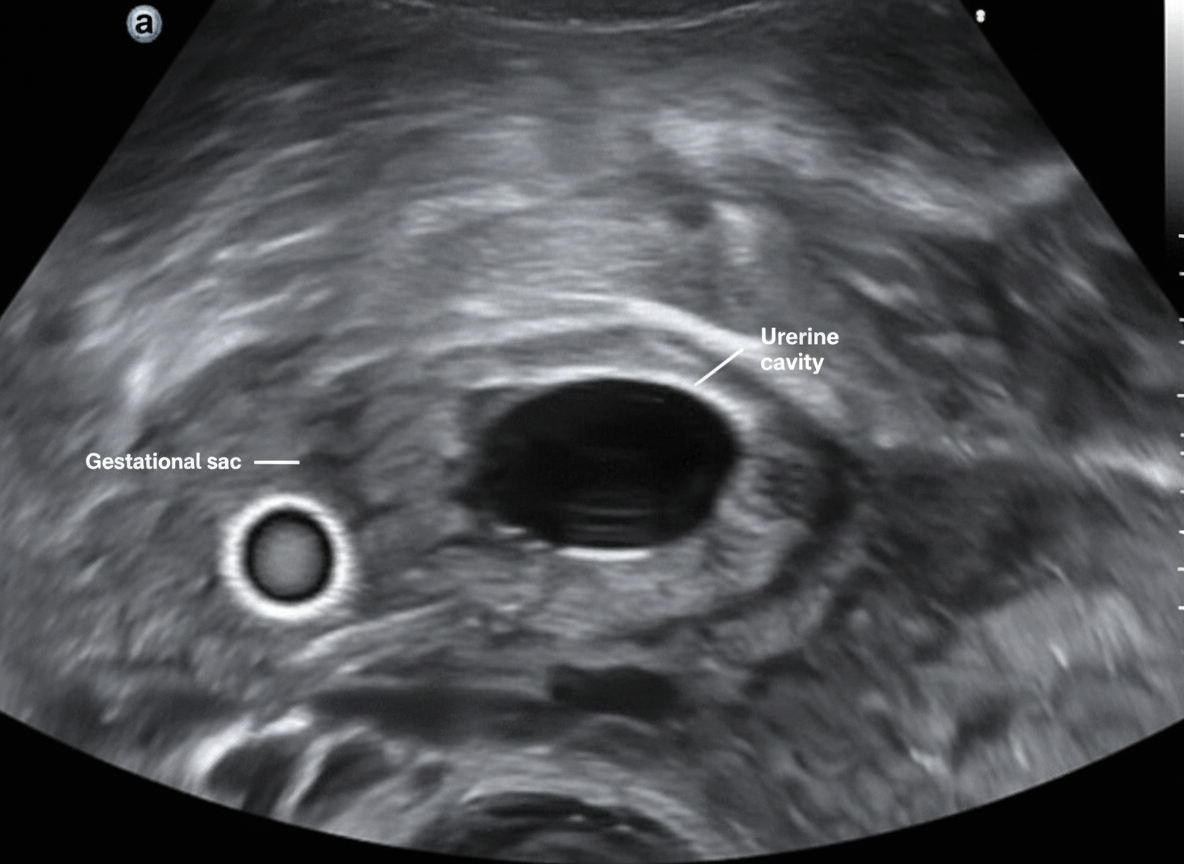
Which of the following conditions can present similarly to an unruptured ectopic pregnancy?
A 35-year-old woman complains of severe lower abdominal pain, which is worst during menstruation. Laparoscopic examination of the pelvis demonstrates multiple small brown spots on the surface of pelvic structures. Biopsy of one of the lesions reveals glandular tissue resembling normal endometrium with no cytologic atypia or abnormally shaped glands. Which of the following is the most likely diagnosis?
What is the mechanism responsible for high rates of spontaneous abortion in a septate uterus?
Which of the following conditions is not a classic major risk factor for the pathology shown in the ultrasound image?
Which of the following is NOT a feature of Mayer Rokitansky Kuster Hauser syndrome?
Regarding vaginal candidiasis, which of the following statements is FALSE?
Vulval candidiasis is associated with:
Practice by Chapter
Abnormal Uterine Bleeding
Practice Questions
Endometriosis
Practice Questions
Adenomyosis
Practice Questions
Uterine Fibroids
Practice Questions
Ovarian Cysts
Practice Questions
Pelvic Inflammatory Disease
Practice Questions
Vulvovaginitis
Practice Questions
Pelvic Organ Prolapse
Practice Questions
Vulvar Disorders
Practice Questions
Benign Breast Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app