
Gynecological Disorders — MCQs

On this page
Upon hysteroscopy, which of the following cannot be visualized?
A middle-aged woman presents with a fishy-smelling vaginal discharge and 'clue cells' are observed on a wet preparation. What is the most likely diagnosis?
A lesion in a female child born to a mother treated with diethylstilbestrol (DES) is most likely to be?
Which of the following fibroids are not suitable for uterine artery embolization?
Females with vaginal atresia are characterized by all of the following except?
Red degeneration of a fibroid is primarily due to which of the following pathological processes?
A 35-year-old patient presents with a 3 x 4 cm clear ovarian cyst on right side as noted on ultrasound. What is the next line of management?
Which of the following findings most strongly indicates a sizable intra-abdominal hemorrhage in a ruptured ectopic pregnancy?
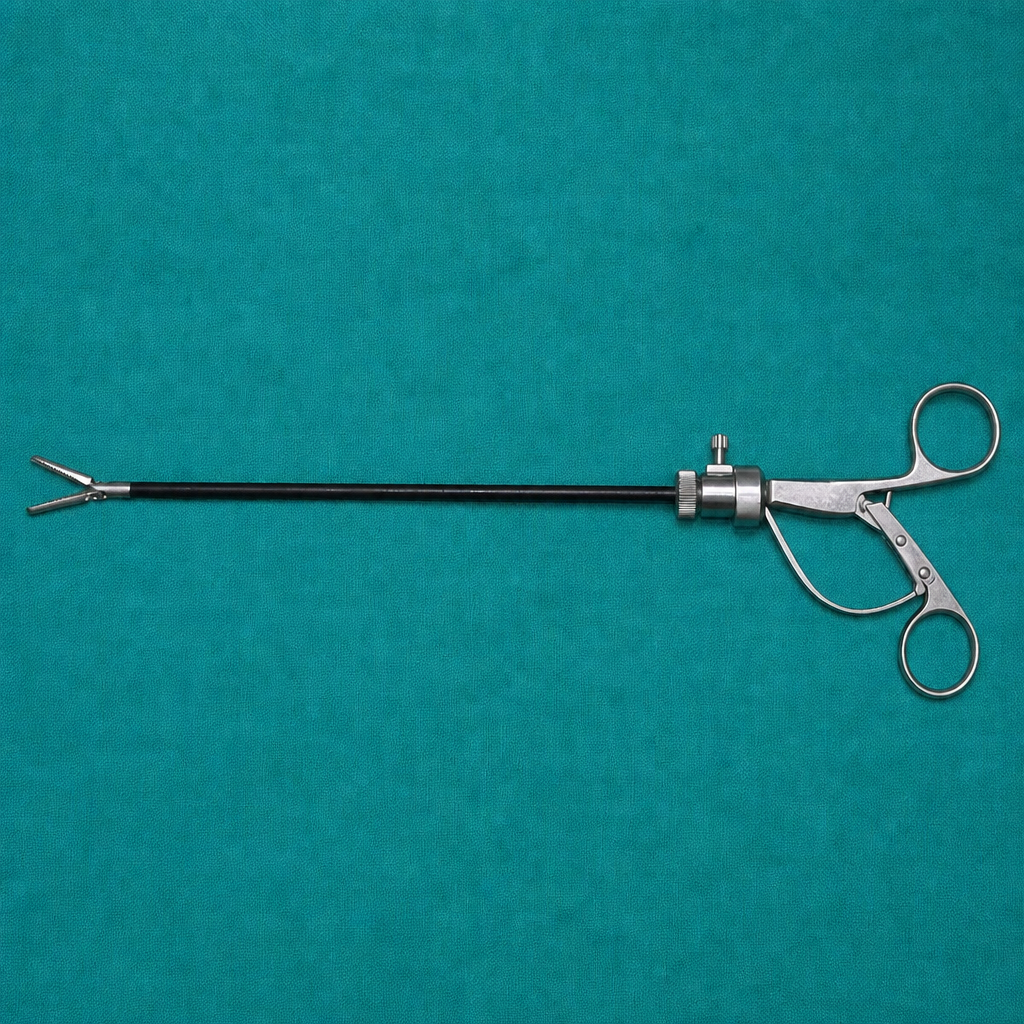
The instrument shown in the image is used for which of the following procedures?
Endometrial implants are deficient in which enzyme?
Practice by Chapter
Abnormal Uterine Bleeding
Practice Questions
Endometriosis
Practice Questions
Adenomyosis
Practice Questions
Uterine Fibroids
Practice Questions
Ovarian Cysts
Practice Questions
Pelvic Inflammatory Disease
Practice Questions
Vulvovaginitis
Practice Questions
Pelvic Organ Prolapse
Practice Questions
Vulvar Disorders
Practice Questions
Benign Breast Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app