
Gynecological Disorders — MCQs

On this page
After treatment of ectopic pregnancy with methotrexate, at what intervals are hCG levels typically checked?
Maximum chances of ureteric injury are associated with which gynecological procedure?
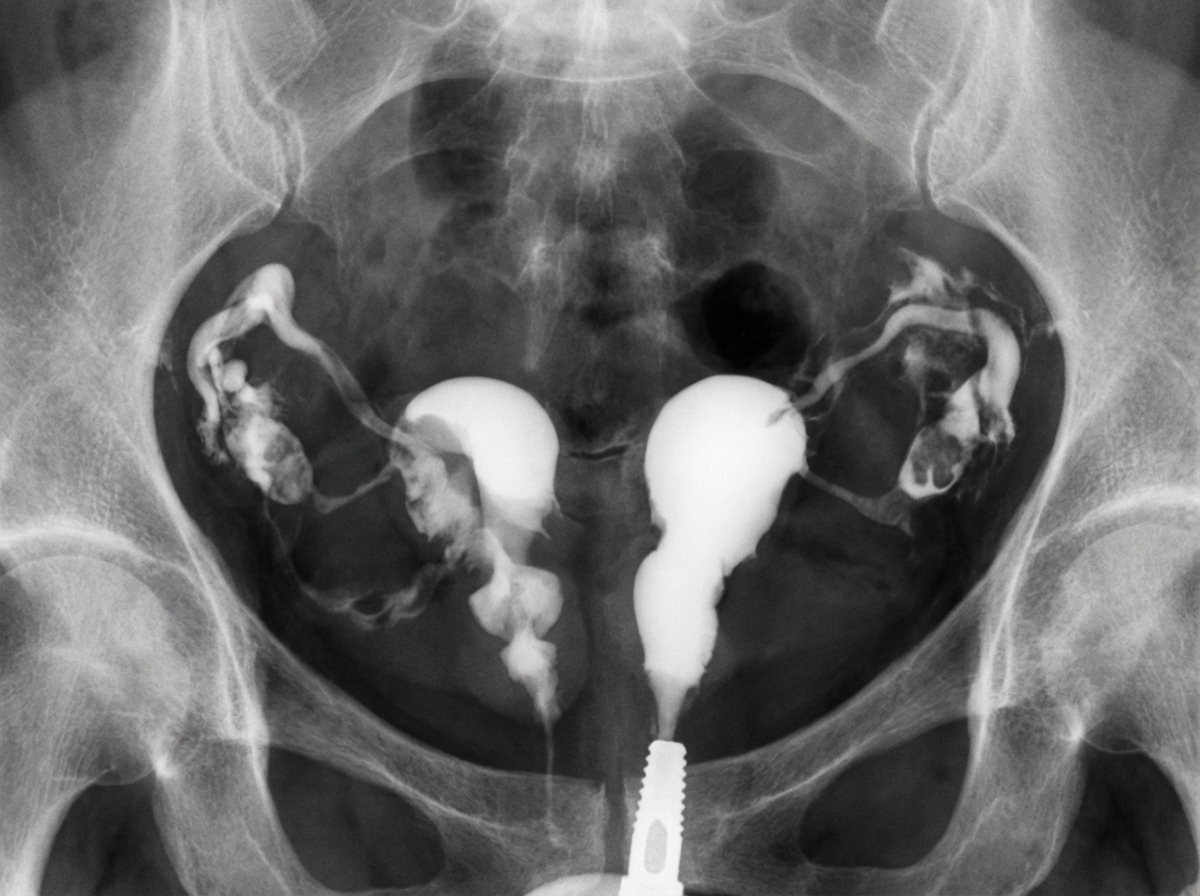
The provided Hysterosalpingogram image demonstrates which of the following uterine anomalies? (Clinical examination confirmed two completely separate cervices and a longitudinal vaginal septum; MRI confirmed two fully separate uterine bodies with a deep intervening fundal cleft.)
What are the diagnostic criteria for ovarian pregnancy?
Which location of ectopic pregnancy is associated with the longest duration before diagnosis?
What is the most frequent symptom of adenomyosis?
Which of the following is NOT true regarding Hyskon used as a distending medium in hysteroscopy?
Clue cells are characteristic findings in which of the following conditions?
Which of the following is NOT a feature of Bacterial vaginosis?
Regarding clue cells, all are true except?
Practice by Chapter
Abnormal Uterine Bleeding
Practice Questions
Endometriosis
Practice Questions
Adenomyosis
Practice Questions
Uterine Fibroids
Practice Questions
Ovarian Cysts
Practice Questions
Pelvic Inflammatory Disease
Practice Questions
Vulvovaginitis
Practice Questions
Pelvic Organ Prolapse
Practice Questions
Vulvar Disorders
Practice Questions
Benign Breast Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app