
Gynecological Disorders — MCQs

On this page
Endometriosis is commonly associated with which of the following?
A 16-year-old girl presents with lower abdominal pain and fever. On physical examination, a tender adnexal mass is felt. Further questioning in private reveals that she has a new sexual partner, her periods are irregular, and she has a vaginal discharge. Which of the following test results is most likely to be seen in this scenario?
Which organism contributes to the vaginal defense mechanism?
Which of the following statements is FALSE regarding laparoscopic hysterectomy?
Which hormone is primarily responsible for maintaining the vaginal defense mechanism?
What is the most common cause of pelvic inflammatory disease in virgin girls?
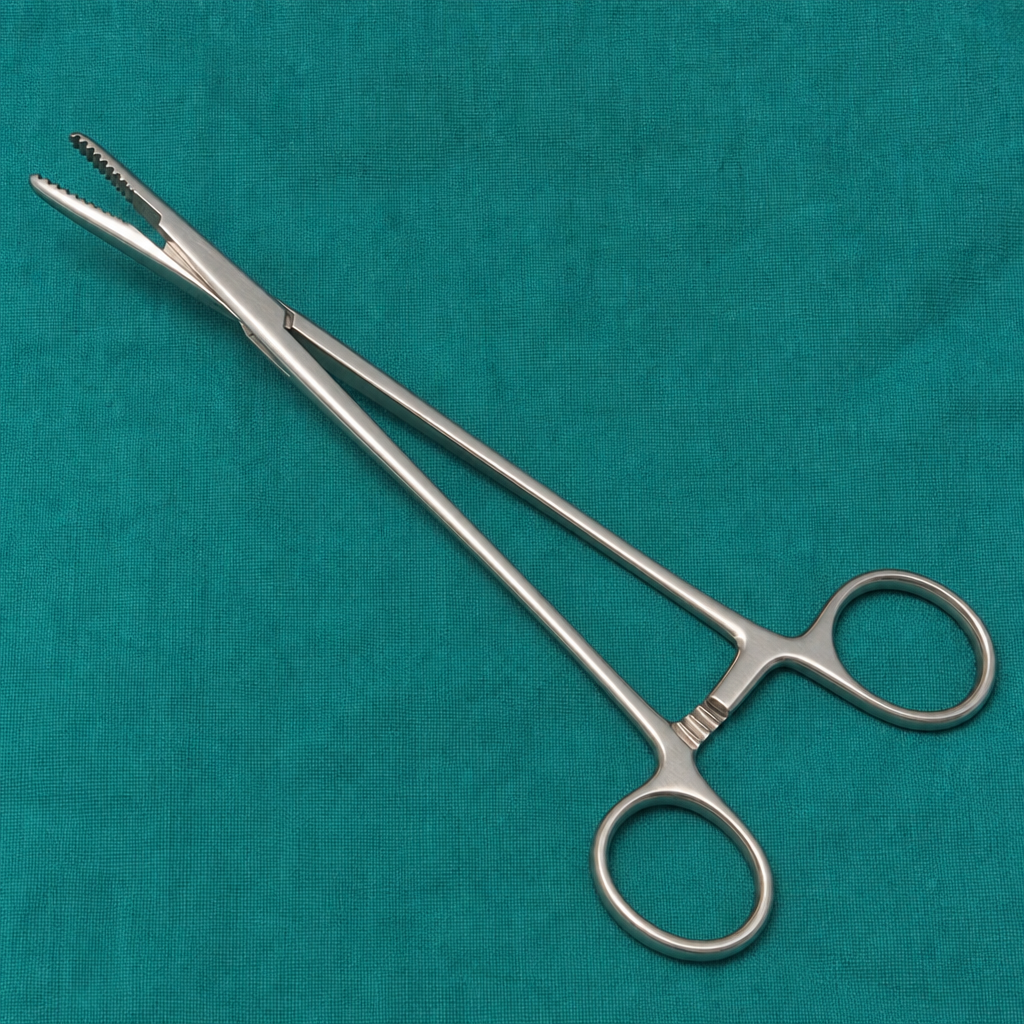
Which instrument is shown below?
A 35-year-old patient's ultrasound shows a 3x4 cm simple ovarian cyst on the right side. What is the next line of management?
Gartner's duct cyst is associated with all of the following except?
All of the following may be associated with a uterine fibroid except?
Practice by Chapter
Abnormal Uterine Bleeding
Practice Questions
Endometriosis
Practice Questions
Adenomyosis
Practice Questions
Uterine Fibroids
Practice Questions
Ovarian Cysts
Practice Questions
Pelvic Inflammatory Disease
Practice Questions
Vulvovaginitis
Practice Questions
Pelvic Organ Prolapse
Practice Questions
Vulvar Disorders
Practice Questions
Benign Breast Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app