
Gynecological Disorders — MCQs

On this page
A 13-year-old girl presents with acute lower abdominal pain. She has a history of cyclical pain for the past six months and has not yet attained menarche. On local genital examination, a tense bulge is seen in the region of the hymen. What is the most probable diagnosis?
What is the most common congenital abnormality of the uterus?
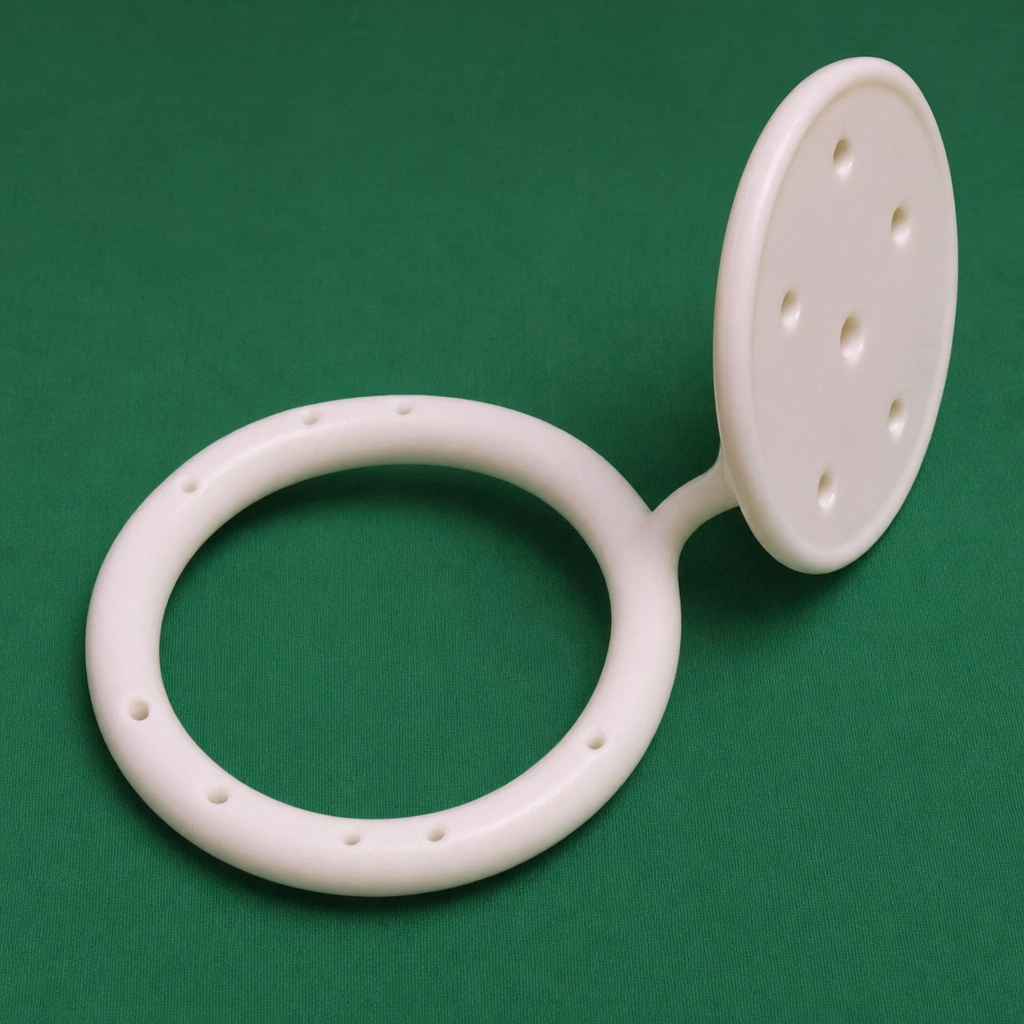
The pessary shown in the figure is used for which of the following conditions?
Which of the following is true about the pathophysiology of uterine fibroids?
A 25-year-old married woman with regular menstruation presents with fever, lower abdominal pain, and dysmenorrhea. On examination, there are bilateral soft tender masses of 3 cm diameter in both fornices, and the uterus is of normal size. What is the most likely diagnosis?
What is the critical mitogen for uterine fibroid growth?
The transformation zone moves out under the influence of all except:
What is the most common cause of hematocolpos?
During laparoscopy, what is the preferred site for obtaining cultures in a patient with acute pelvic inflammatory disease (PID)?
Repeated curettage is most likely to lead to which of the following conditions?
Practice by Chapter
Abnormal Uterine Bleeding
Practice Questions
Endometriosis
Practice Questions
Adenomyosis
Practice Questions
Uterine Fibroids
Practice Questions
Ovarian Cysts
Practice Questions
Pelvic Inflammatory Disease
Practice Questions
Vulvovaginitis
Practice Questions
Pelvic Organ Prolapse
Practice Questions
Vulvar Disorders
Practice Questions
Benign Breast Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app