
Gynecological Disorders — MCQs

On this page
A sexually active female presenting with profuse frothy foul-smelling discharge with intense itching. Strawberry cervix revealed on examination. What will be the diagnosis?
45 years female with 3 months of menorrhagia. USG showing 2 cm submucosal fibroid. What is the most appropriate management option?
Which of the following treatments is used for vulvar atrophy and itching?
Green frothy vaginal discharge is produced by –
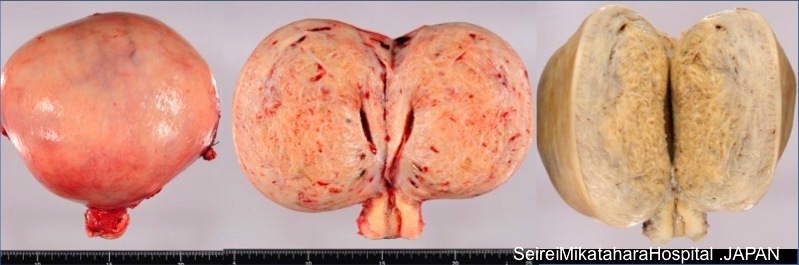
A 30-year-old woman presents with complaints of dysmenorrhea and dyspareunia, accompanied by chronic pelvic pain. She undergoes a hysterectomy. Based on the cut section of the hysterectomy specimen provided, identify the condition.
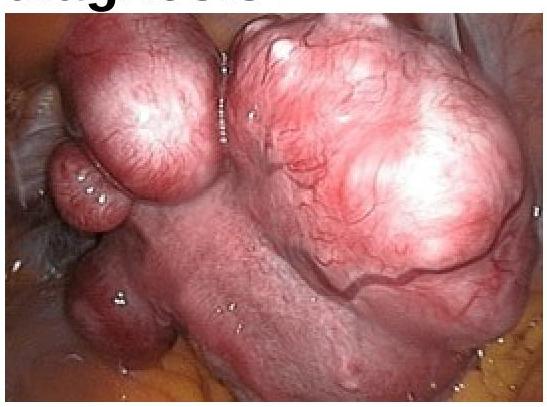
In a woman complaining of AUB following image was seen in endoscopic examination of uterus. What will be the diagnosis?
What is the most reliable method to confirm the correct placement of a ring pessary in a patient with uterine prolapse?
Long-standing pelvic inflammatory disease (PID) may lead to which of the following complications?
Dilatation & curettage (D&C) is contraindicated in-
What type of uterine anomaly is shown in this X-ray HSG image?

Practice by Chapter
Abnormal Uterine Bleeding
Practice Questions
Endometriosis
Practice Questions
Adenomyosis
Practice Questions
Uterine Fibroids
Practice Questions
Ovarian Cysts
Practice Questions
Pelvic Inflammatory Disease
Practice Questions
Vulvovaginitis
Practice Questions
Pelvic Organ Prolapse
Practice Questions
Vulvar Disorders
Practice Questions
Benign Breast Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app