
Gynecological Disorders — MCQs

On this page
Where are Gartner's cysts typically located?
What is the treatment of choice for a Bartholin cyst?
What factor is associated with decreased success in the medical management of ectopic pregnancy?
A 16-year-old girl presents with cyclical pelvic pain every month. She has not achieved menarche yet. On examination, a suprapubic bulge can be seen in the lower abdomen. PR examination reveals a bulging swelling in the anterior aspect. What is the most likely diagnosis?
In your STI clinic, standardized treatment kits are available for different conditions based on clinical presentation and likely pathogens. A 22-year-old female comes to the STI clinic with minimal vaginal discharge. On speculum examination, erosions are seen on the cervix. Which of the following treatment kit should be given to this patient?
A woman comes with complaints of pain and swelling in the perineal area. She also has complaints of difficulty in walking and sitting. She gives a history of multiple sexual partners. On examination, a tender swelling is seen with redness on the labia. What is the most likely diagnosis?
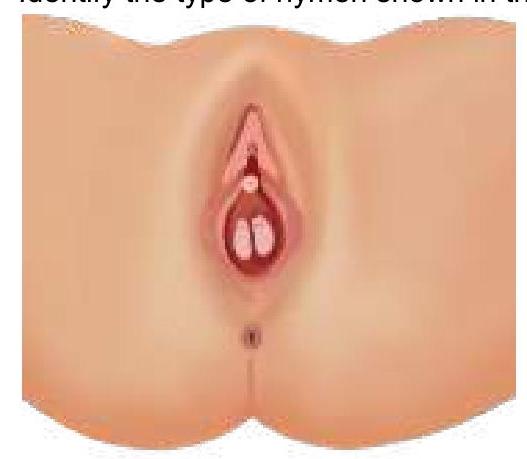
Identify the type of hymen.
What is the best treatment option for a septate uterus?
A mother brought her 16-year-old daughter to Gynaecology OPD with a complaint of not attending menarche. She gives a history of cyclic abdominal pain. On further examination, a midline abdominal swelling is seen. Per rectal examination reveals a bulging mass in the vaginal area. Which of the following can be most commonly seen?
60-year-old female with a history of intermittent bleeding. What is the diagnosis based on the ultrasound image?

Practice by Chapter
Abnormal Uterine Bleeding
Practice Questions
Endometriosis
Practice Questions
Adenomyosis
Practice Questions
Uterine Fibroids
Practice Questions
Ovarian Cysts
Practice Questions
Pelvic Inflammatory Disease
Practice Questions
Vulvovaginitis
Practice Questions
Pelvic Organ Prolapse
Practice Questions
Vulvar Disorders
Practice Questions
Benign Breast Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app