
Gynecological Disorders — MCQs

On this page
Which of the following is TRUE regarding bacterial vaginosis?
A 30-year-old woman presents with vaginal discharge and lower abdominal pain for 10 days. Examination reveals cervical motion tenderness and adnexal tenderness. Laboratory tests show elevated WBC count. What is the most appropriate initial antibiotic regimen?
Why does Chlamydia trachomatis infection often remain asymptomatic in women?
What is the preferred management of a uterine septum?
The patient presented with a retroverted uterus, dysmenorrhea, and dyspareunia. What is the next step of the investigation?
What are clue cells?
A patient complained of whitish discharge from the vagina and yellow staining on their clothes. There is no itching, no redness, and pH is acidic. What is the likely cause?
A woman presents with painless ulcers on the vulva, she gives a history of having multiple sexual partners and has had a stillbirth at 28 weeks in the past. What is the next best step of investigation?
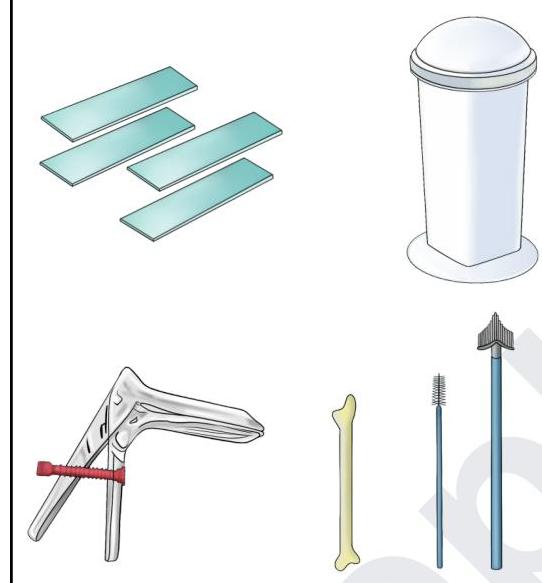
The following set of instruments are used for which procedure?
A female patient having frothy vaginal discharge was found to have a strawberry cervix. Which of the following is the drug of choice?
Practice by Chapter
Abnormal Uterine Bleeding
Practice Questions
Endometriosis
Practice Questions
Adenomyosis
Practice Questions
Uterine Fibroids
Practice Questions
Ovarian Cysts
Practice Questions
Pelvic Inflammatory Disease
Practice Questions
Vulvovaginitis
Practice Questions
Pelvic Organ Prolapse
Practice Questions
Vulvar Disorders
Practice Questions
Benign Breast Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app