
Gynecologic Oncology — MCQs

On this page
What is the co-test in cervical cancer screening?
Which is the primary chemotherapeutic agent used for cervical cancer?
A patient presents with an endometrial thickness of 14mm with an adnexal mass. She has a history of complex endometrial hyperplasia with the presence of atypical cells. Which of the following is likely the diagnosis?
Which type of hysterectomy is done in a case of carcinoma cervix stage IB?
A woman diagnosed with cervical cancer is found to have unilateral hydroureteronephrosis on imaging due to tumor invasion. What is the FIGO stage of her disease?
A 62-year-old postmenopausal woman with a history of hypertension presents with vaginal bleeding. Her blood pressure is 170 / 100 mmHg. What is the most appropriate next step in management?
A 65-year-old postmenopausal woman presents with painless vaginal bleeding. She has no history of hormone replacement therapy. What is the most likely diagnosis?
A patient presents with ascites and omental caking. Imaging reveals solid components in an adnexal mass, and there is a long-standing history of symptoms. CA-125 is positive. What is the most probable diagnosis?
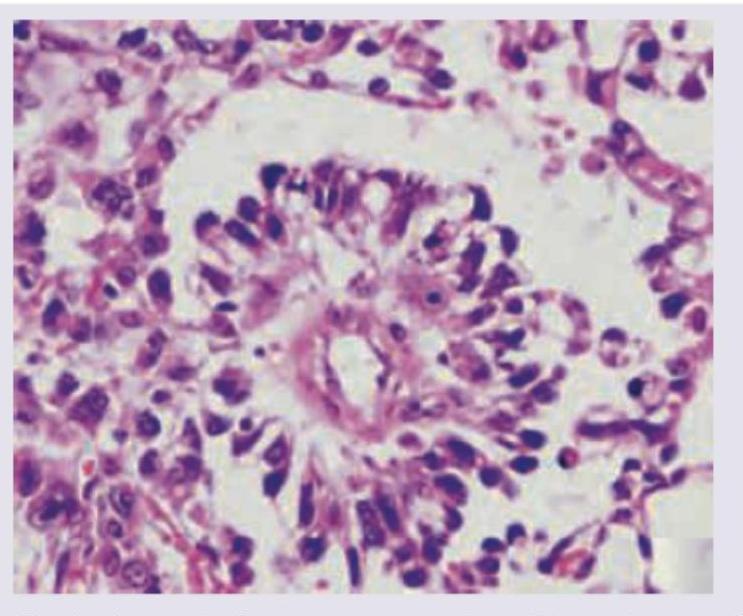
15-year-old girl presents with a big pelvic mass. CT abdomen shows omental thickening and large ovarian mass. For surgical staging, biopsy of the ovarian mass was done. The specimen findings are diagnostic of?
Bilateral total salpingectomy is a recommended surgical procedure to reduce the risk of :
Practice by Chapter
Cervical Cancer
Practice Questions
Endometrial Cancer
Practice Questions
Ovarian Cancer
Practice Questions
Vulvar and Vaginal Cancer
Practice Questions
Gestational Trophoblastic Disease
Practice Questions
Screening for Gynecologic Cancers
Practice Questions
Principles of Gynecologic Oncology Surgery
Practice Questions
Radiation Therapy in Gynecologic Malignancies
Practice Questions
Chemotherapy in Gynecologic Oncology
Practice Questions
Palliative Care in Gynecologic Oncology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app