
Gynecologic Oncology — MCQs

On this page
Which one of the following is NOT a mandatory procedure for FIGO staging of Carcinoma cervix?
Consider the following statements regarding Carcinoma Cervix: 1. Clinical staging is done 2. Treatment if provided in stage I leads to survival rate of 80–90 % 3. Surgery is preferred in young women with stage III disease 4. HPV is considered to be the causative agent Which of the statements given above are correct?
Which of the following are the vaccines for prevention of cervical cancer? 1. Cervarix 2. Gardasil 3. T-dap 4. Influenza Select the correct answer using the code given below:
The most common site of cervical cancer is:
Tumor marker of epithelial ovarian carcinoma is:
What is the age group distribution for vulval cancer?
A 37-year-old unmarried nulliparous woman, having regular intercourse, is on oral contraceptive pills. Her mother was diagnosed with carcinoma breast at 60 years of age, and her elder sister was diagnosed with carcinoma ovary at 40 years of age. What is the next line of management?
The following set of instruments are used for which procedure?
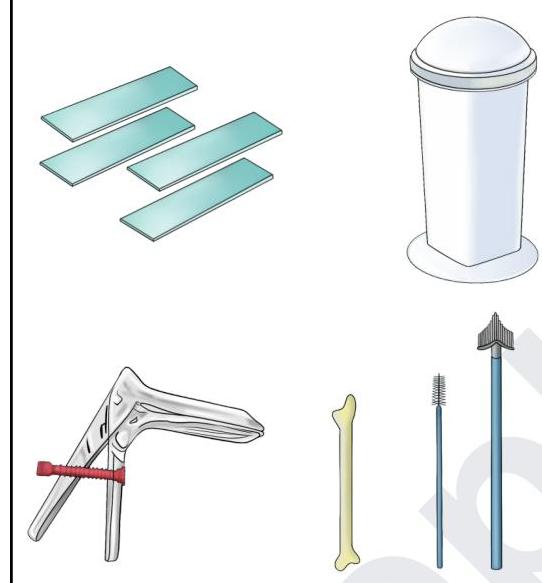
Arrange the following in sequential order with regards to the steps of collection of samples for pap smear testing: Use posterior vaginal wall retractor Take the sample Make smear on a slide Fix the smear
A 32-year-old HIV-positive woman with CD4 count 180/µL presents with extensive genital warts resistant to conventional therapy. Recent Pap smear shows HSIL. Which management approach is most appropriate?
Practice by Chapter
Cervical Cancer
Practice Questions
Endometrial Cancer
Practice Questions
Ovarian Cancer
Practice Questions
Vulvar and Vaginal Cancer
Practice Questions
Gestational Trophoblastic Disease
Practice Questions
Screening for Gynecologic Cancers
Practice Questions
Principles of Gynecologic Oncology Surgery
Practice Questions
Radiation Therapy in Gynecologic Malignancies
Practice Questions
Chemotherapy in Gynecologic Oncology
Practice Questions
Palliative Care in Gynecologic Oncology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app