
Gynecologic Oncology — MCQs

On this page
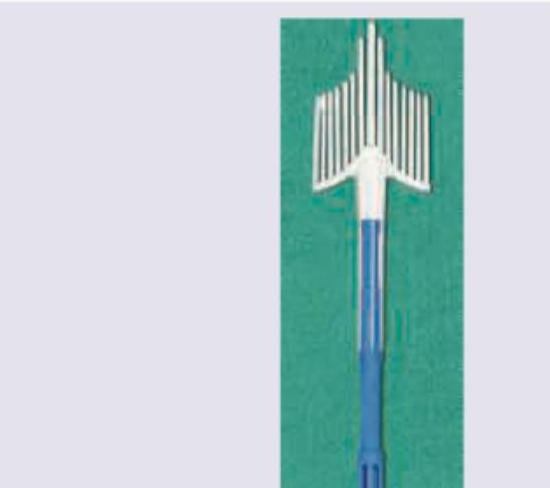
Identify the gynecological instrument shown below. (Recent Neet Pattern 2016-17)
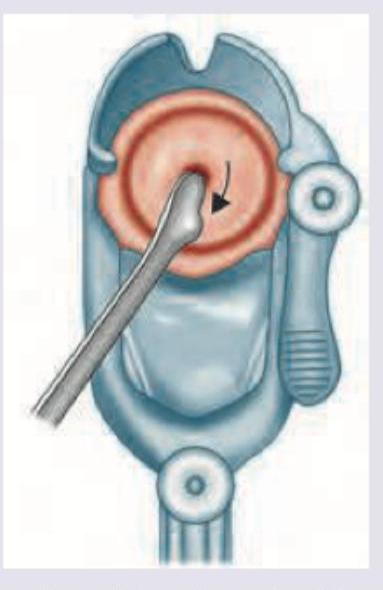
The procedure shown below is called:
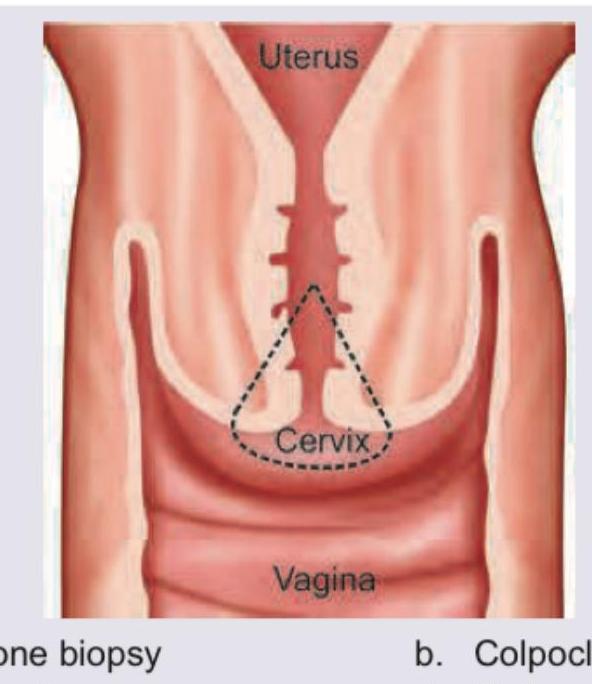
All are true about the procedure being performed except: (Recent Neet Pattern 2016-17)
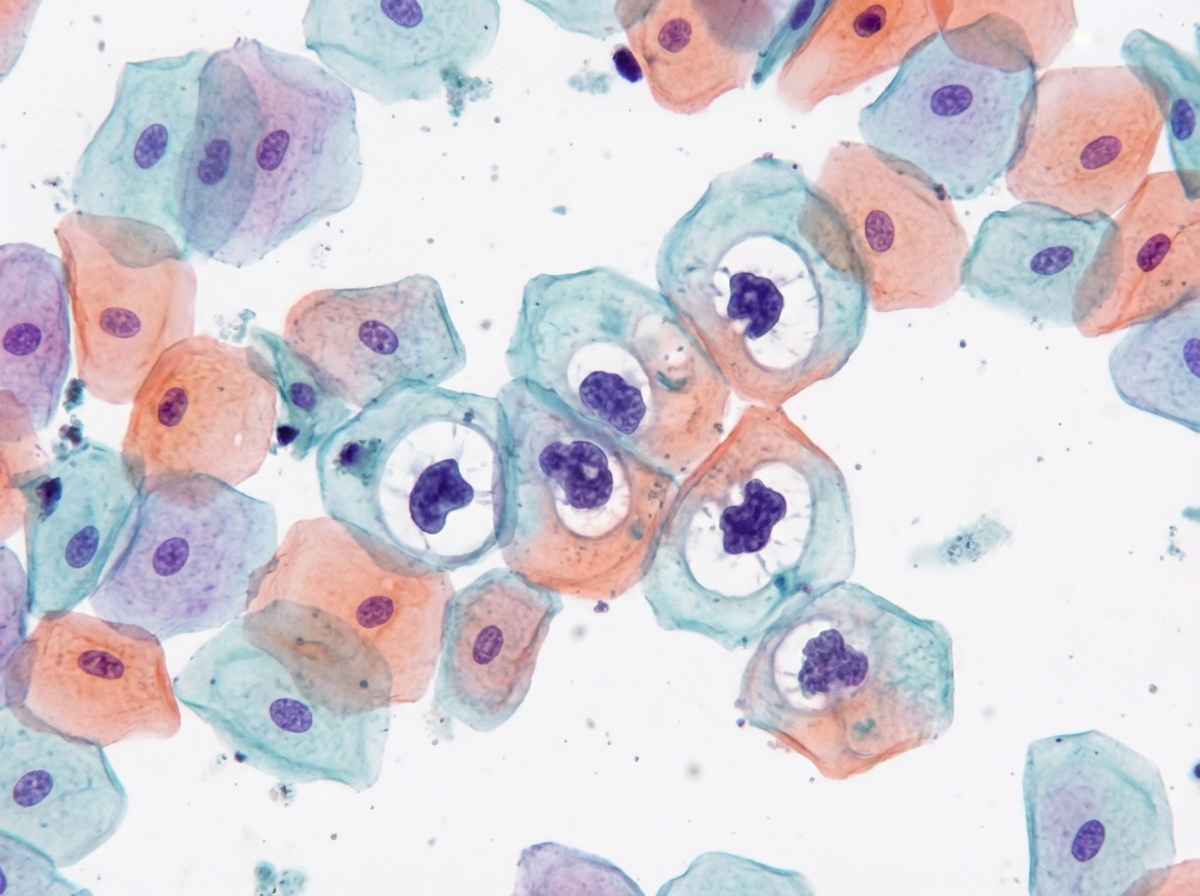
A woman in the late menstrual phase presents with an ovarian mass. Her Pap smear shows predominantly superficial cells stained orange (see image). What is the most likely ovarian tumor?
Which one of the following is an indication for knife conisation? 1. Treatment of Nabothian follicle 2. Diagnosis and directed biopsy of cervix when punch biopsy is inadequate 3. Unsatisfactory colposcopy (transformation zone not fully visible) 4. Negative endocervical curettage Select the correct answer using the code given below:
Bilateral total salpingectomy is a recommended surgical procedure to reduce the risk of :
Prophylactic oophorectomy is recommended in high risk women with which of the following ? 1. Carrying BRCA1 or BRCA2 genes 2. Family history of breast, colon, ovarian cancer 3. Patients having tubo-ovarian abscess Select the correct answer using the code given below :
Which of the following are indications of cold knife conization? 1. Inconsistent findings between colposcopy, cytology and directed biopsy 2. Persistent CIN-1 lesion in women willing for future fertility 3. Carcinoma in situ 4. Unsatisfactory colposcopic finding where the entire margin of lesion is not visible Select the correct answer using the code given below.
Which one of the following drugs is most effective in the treatment of gestational trophoblastic neoplasia?
Which of the following are favourable factors in prognosis of ovarian malignancy? 1. Older age group 2. Well-differentiated tumour 3. Smaller tumour volume 4. Younger age group Select the correct answer using the code given below.
Practice by Chapter
Cervical Cancer
Practice Questions
Endometrial Cancer
Practice Questions
Ovarian Cancer
Practice Questions
Vulvar and Vaginal Cancer
Practice Questions
Gestational Trophoblastic Disease
Practice Questions
Screening for Gynecologic Cancers
Practice Questions
Principles of Gynecologic Oncology Surgery
Practice Questions
Radiation Therapy in Gynecologic Malignancies
Practice Questions
Chemotherapy in Gynecologic Oncology
Practice Questions
Palliative Care in Gynecologic Oncology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app