
Gynecologic Oncology — MCQs

On this page
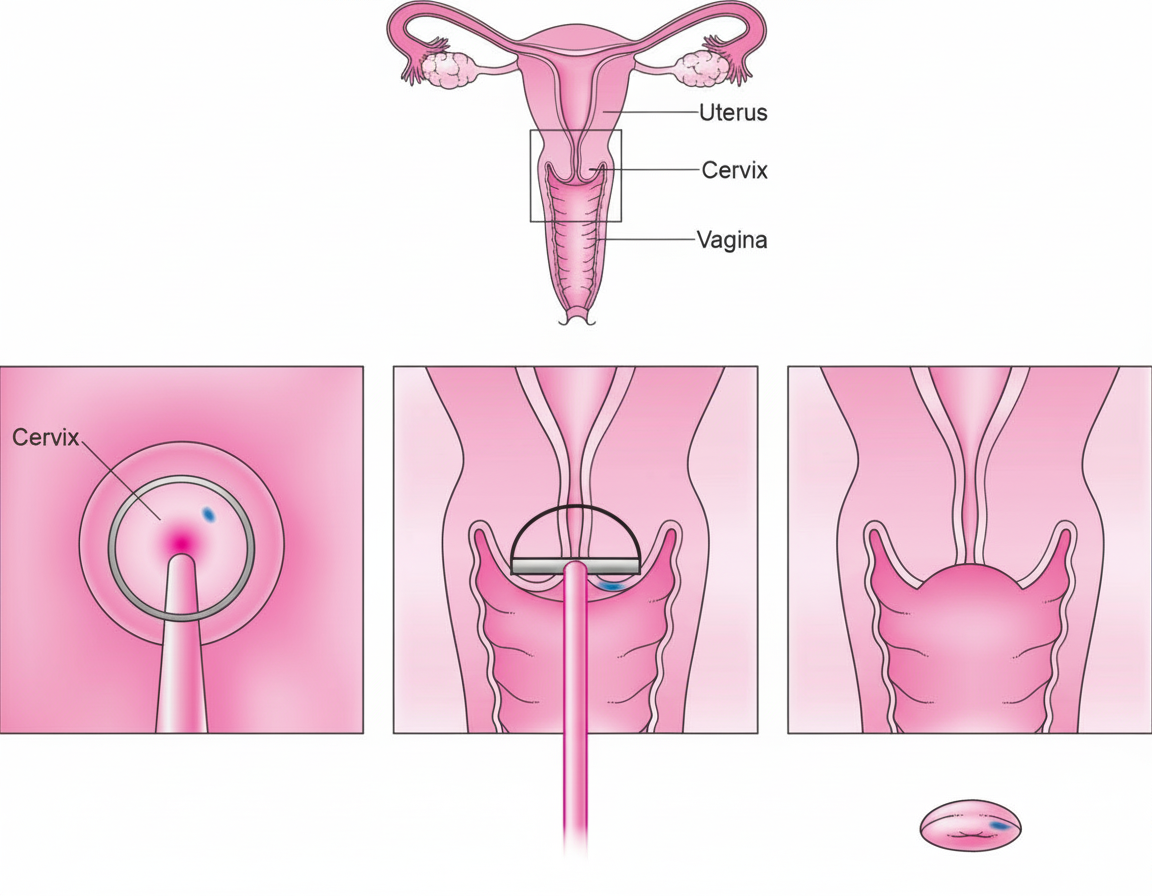
The procedure shown below is
What is the commonest tumor of the ovary occurring in a young woman?
What is the treatment of choice for hydatiform mole with a uterine size of 28 weeks?
All are signs of inoperability of carcinoma of the cervix except?
What is the percentage change of cystic glandular hyperplasia turning to malignancy?
A 38-year-old woman with a history of multiple sexual partners is most at risk for which of the following?
Intrauterine exposure of diethylstilbestrol is associated with which of the following conditions?
A woman presents with a 12-week pregnancy complaining of excessive vomiting and mild vaginal bleeding for two weeks. Her fundal height measures 16 weeks, and the cervical os is closed. An ultrasound reveals a snowstorm appearance in part of the uterus along with a fetus measuring 10 weeks crown-rump length. Fetal heart activity is absent. What is the best management option?
Which of the following is the most common form of persistent trophoblastic disease that follows a non-molar pregnancy?
A 38-year-old female has a Pap smear suggestive of HSIL. Colposcopy-directed biopsy can reveal all of the following, EXCEPT:
Practice by Chapter
Cervical Cancer
Practice Questions
Endometrial Cancer
Practice Questions
Ovarian Cancer
Practice Questions
Vulvar and Vaginal Cancer
Practice Questions
Gestational Trophoblastic Disease
Practice Questions
Screening for Gynecologic Cancers
Practice Questions
Principles of Gynecologic Oncology Surgery
Practice Questions
Radiation Therapy in Gynecologic Malignancies
Practice Questions
Chemotherapy in Gynecologic Oncology
Practice Questions
Palliative Care in Gynecologic Oncology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app