
Gynecologic Oncology — MCQs

On this page
A young lady presents with mild erosion of the cervix and a Pap smear shows dysplasia. What is the next step in management?
A 45-year-old woman presents to the gynecology department with prolonged vaginal bleeding. On examination, a cervical lesion is found that bleeds on touch. Her past history is insignificant. She had a Pap smear approximately 10 years ago, which was normal. What is the next best investigation?
What condition is characterized by a 'snow storm' appearance on ultrasound (IJSG)?
What is the chemotherapy regimen for dysgerminoma?
Following molar pregnancy evacuation, in which timeframe do post-treatment HCG levels typically normalize?
What is the most common ovarian malignancy in the post-menopausal period?
A 62-year-old postmenopausal woman presents with a blood-tinged vaginal discharge. Her last menstrual period was 10 years ago. On bimanual pelvic examination, the uterus is normal in size, with no palpable adnexal masses. There are no cervical erosions or masses. Her body mass index is 33. She has a 30-year history of hypertension and type 2 diabetes mellitus. An endometrial biopsy specimen is most likely to show which of the following?
What is the first change observed on colposcopy in a precancerous lesion?
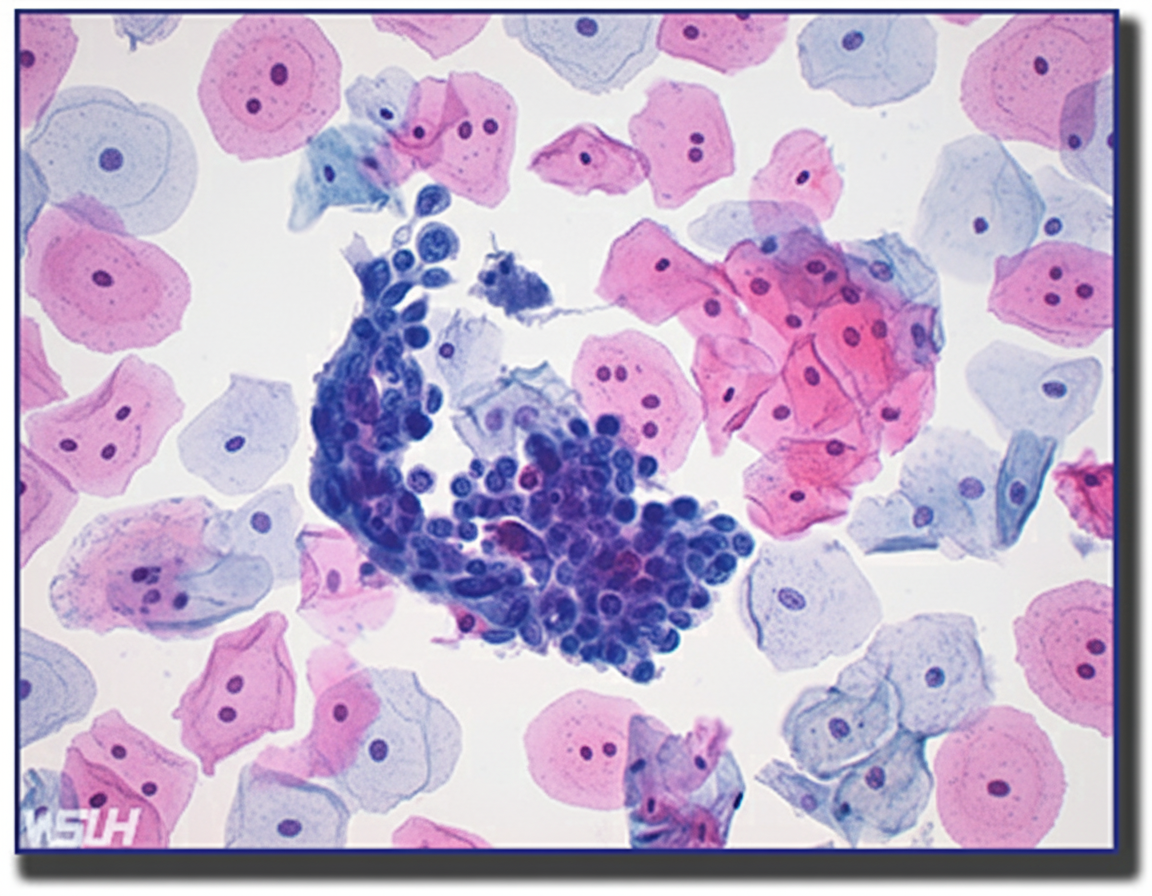
A 30-year-old woman's Pap smear results are provided below. What is your next recommended approach?
A 53-year-old woman with an ovarian tumor presents with breathlessness and right-sided chest pain. The chest X-ray shows obliteration of the right costophrenic angle. What is the most likely diagnosis?
Practice by Chapter
Cervical Cancer
Practice Questions
Endometrial Cancer
Practice Questions
Ovarian Cancer
Practice Questions
Vulvar and Vaginal Cancer
Practice Questions
Gestational Trophoblastic Disease
Practice Questions
Screening for Gynecologic Cancers
Practice Questions
Principles of Gynecologic Oncology Surgery
Practice Questions
Radiation Therapy in Gynecologic Malignancies
Practice Questions
Chemotherapy in Gynecologic Oncology
Practice Questions
Palliative Care in Gynecologic Oncology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app