
Gynecologic Oncology — MCQs

On this page
What is the treatment of choice for sarcoma botryoides?
What is the stage of carcinoma of the endometrium with invasion of 10 mm of the myometrium?
A 35-year-old woman presents with postcoital bleeding and foul-smelling discharge. What is the most important investigation to arrive at a diagnosis?
A 32-year-old asymptomatic woman has a Pap's smear report of ASCUS. What are the possible management options, excluding one?
A 45-year-old female presents with postcoital bleeding. On per speculum examination, a friable mass is found in the cervix. What is the next step in management?
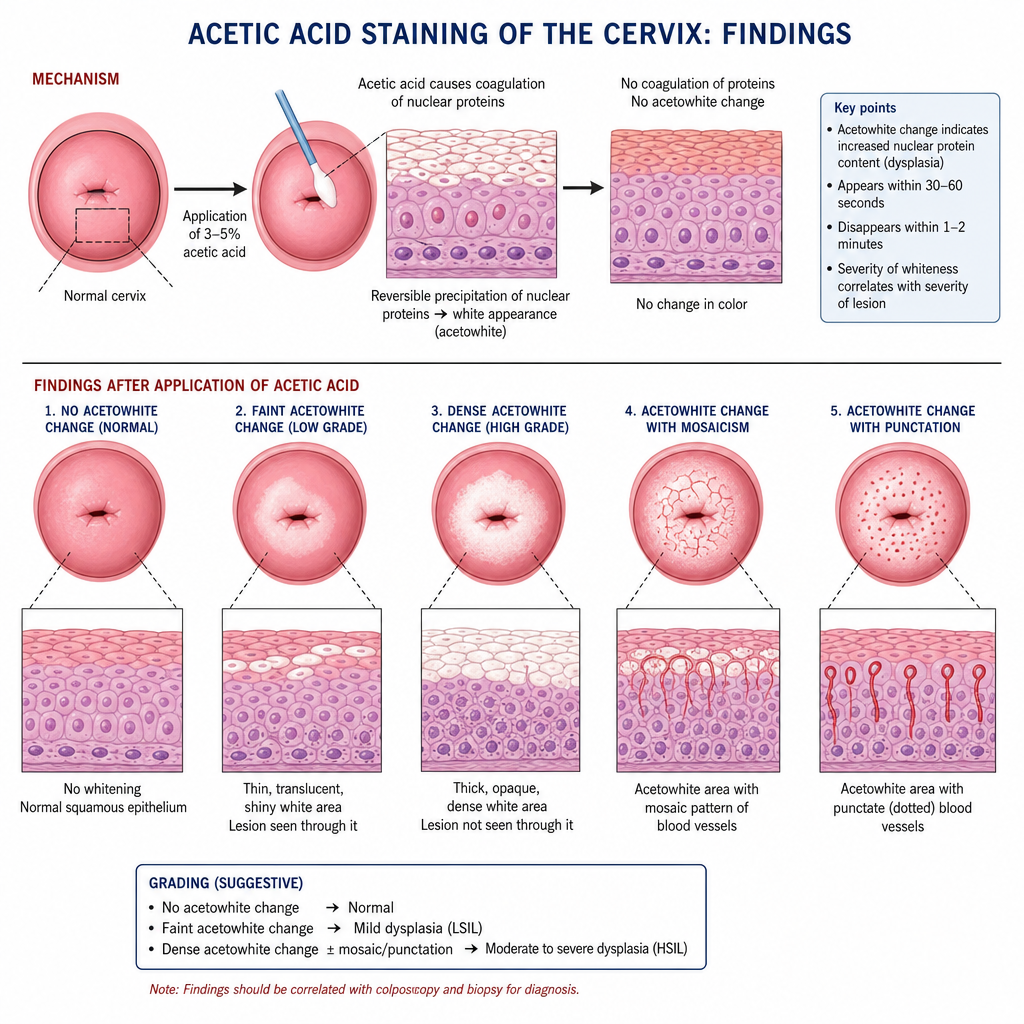
Acetic acid staining of the cervix shows the following findings:
A 41-year-old woman is diagnosed with squamous cell carcinoma of the cervix and has right hydronephrosis evidenced by intravenous pyelogram (IVP). Which of the following statements regarding this patient's condition is most accurate?
Which of the following is not a predisposing factor for carcinoma of the cervix?
Placental alkaline phosphatase is a marker of which of the following?
What is the primary treatment for a lutein cyst associated with a hydatidiform mole?
Practice by Chapter
Cervical Cancer
Practice Questions
Endometrial Cancer
Practice Questions
Ovarian Cancer
Practice Questions
Vulvar and Vaginal Cancer
Practice Questions
Gestational Trophoblastic Disease
Practice Questions
Screening for Gynecologic Cancers
Practice Questions
Principles of Gynecologic Oncology Surgery
Practice Questions
Radiation Therapy in Gynecologic Malignancies
Practice Questions
Chemotherapy in Gynecologic Oncology
Practice Questions
Palliative Care in Gynecologic Oncology
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app