
Fertility and Infertility — MCQs

On this page
Fibroids cause infertility and pregnancy wastage because?
Which of the following locations of tubal obstruction is least amenable to surgical repair?
Which of the following procedures is associated with the maximum chance of re-canalization during surgery for reversal of tubal ligation?
On which day of a normal 28-day menstrual cycle should a hysterosalpingogram be performed for a woman with a 5-day menstrual period?
Recurrent miscarriage is defined as?
What is the initial starting dose of clomiphene citrate for infertility?
Treatment with clomiphene citrate should be limited to how many ovulatory cycles?
Considering the demands of modern life schedules, what is the accepted minimum period of unprotected sexual cohabitation for a couple to be considered infertile?
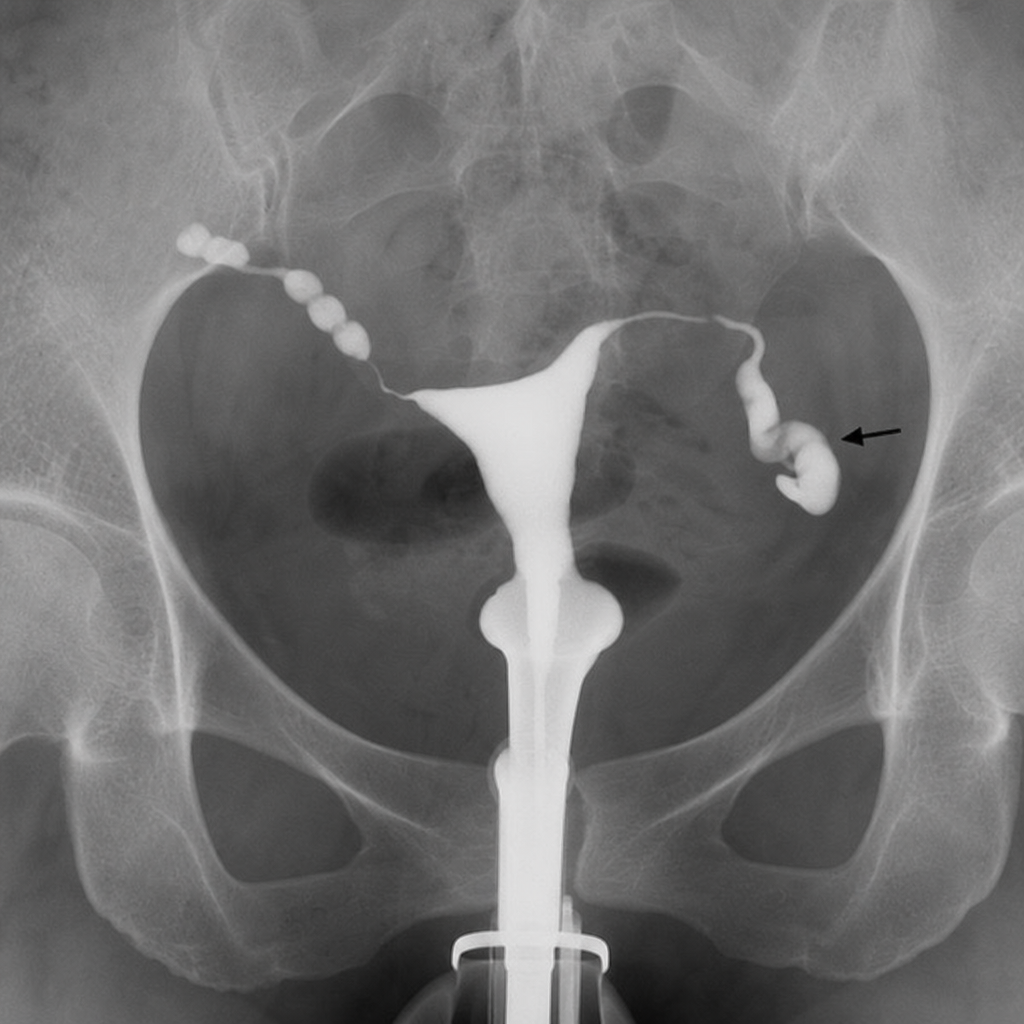
A 38-year-old female presents to the infertility clinic complaining of inability to conceive. Hysterosalpingography was performed, revealing the finding shown. The condition marked by the black arrow is most consistent with which diagnosis, and what is its most common acquired cause?
Which of the following is NOT an essential criterion according to WHO for normal semen analysis?
Practice by Chapter
Reproductive Physiology
Practice Questions
Evaluation of the Infertile Couple
Practice Questions
Male Factor Infertility
Practice Questions
Female Factor Infertility
Practice Questions
Ovulatory Disorders
Practice Questions
Tubal and Peritoneal Factors
Practice Questions
Uterine Factors
Practice Questions
Unexplained Infertility
Practice Questions
Assisted Reproductive Technologies
Practice Questions
Psychological Aspects of Infertility
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app