
Fertility and Infertility — MCQs

On this page
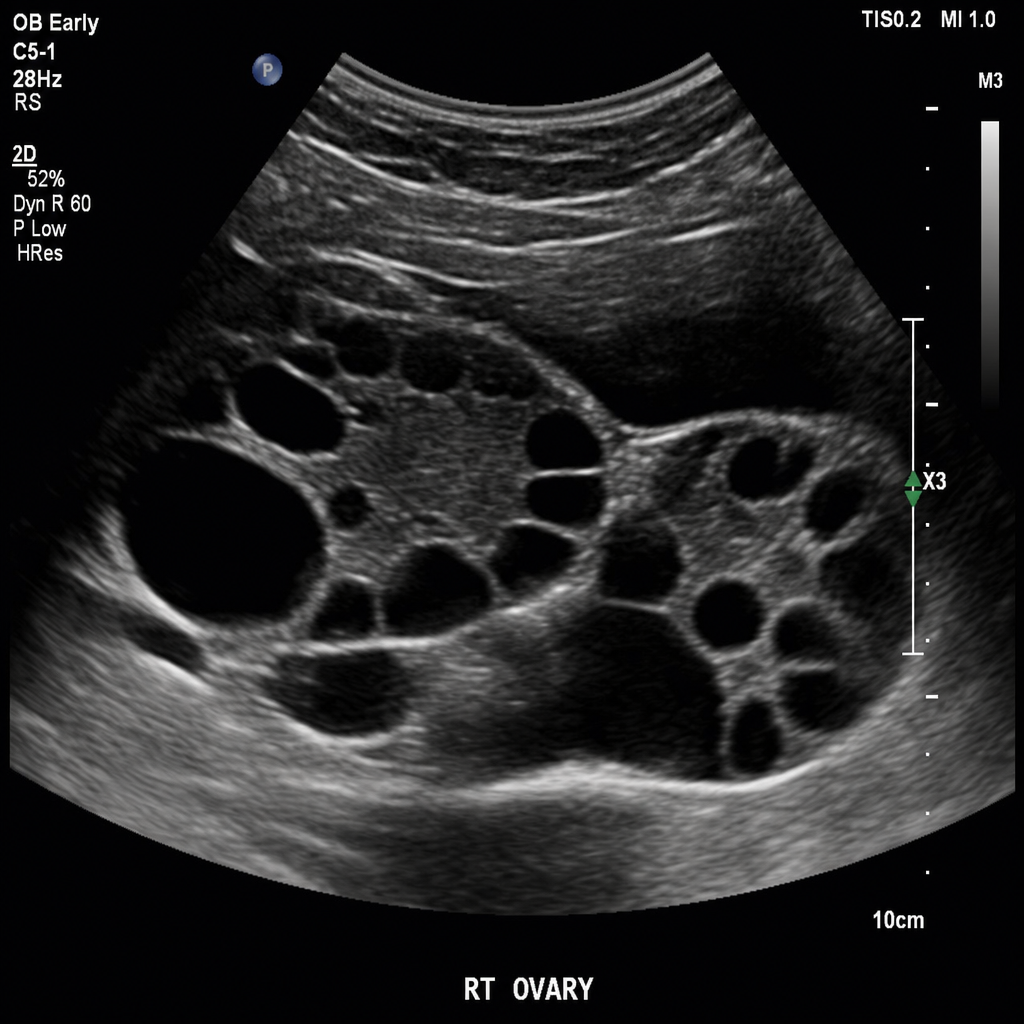
A lady on treatment for infertility developed ascites, abdominal pain, and dyspnea. An ultrasound (USG) of the patient was done. What will be the diagnosis?
In IVF, during cleavage stage embryo transfer, embryos are typically transferred back to uterine cavity at which cell stage?
Abstinence period before semen analysis is?
What is the procedure used in preimplantation genetic diagnosis (PGD) to obtain cells from an embryo for genetic analysis before transferring it to the uterus during IVF?
Endometrial biopsy to detect ovulation is done on which day of the menstrual cycle?
An infertile woman has bilateral tubal block at cornua diagnosed on hysterosalpingography. Next treatment of choice is?
Azoospermic patient can be a father of a child, by which of the following?
In a case of recurrent spontaneous abortion, which of the following investigations is least indicated?
What is the best indicator for ovarian reserve?
Chlamydia trachomatis infection commonly causes: March 2004
Practice by Chapter
Reproductive Physiology
Practice Questions
Evaluation of the Infertile Couple
Practice Questions
Male Factor Infertility
Practice Questions
Female Factor Infertility
Practice Questions
Ovulatory Disorders
Practice Questions
Tubal and Peritoneal Factors
Practice Questions
Uterine Factors
Practice Questions
Unexplained Infertility
Practice Questions
Assisted Reproductive Technologies
Practice Questions
Psychological Aspects of Infertility
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app