
Fertility and Infertility — MCQs

On this page
What is the cause of a twin pregnancy resulting from two different men?
WHO guidelines for minimal sperm count is:
A couple comes for evaluation of infertility. The HSG was normal but semen analysis revealed azoospermia. What is the diagnostic test to differentiate between testicular failure and vas deferens obstruction?
Number of oocytes at birth is
All are steps of GIFT, except:
Asthenospermia means:
Fructose absence in semen analysis suggests:
26 yr lady with delayed cycles presents to the infertility clinic. After diagnosing her to be a case anovulation of 'Normogonadotropic Hypogonadism' type she was put on human menopausal gonadotropin (HMG) for ovulation induction from the second day of her menstrual period. She was 'Triggered' for follicular rupture with Human chorionic gonadotropin (hCG) and on the 19th day of this cycle she developed dyspnoea, reduced urine output, abdominal bloating and pain. What condition is this patient likely suffering from?
A 24-year-old woman with a married life of 4 years visits an infertility clinic with a history of recurrent abortion. On further workup, she is found to have a septate uterus. Which surgery has the best reproductive outcome?
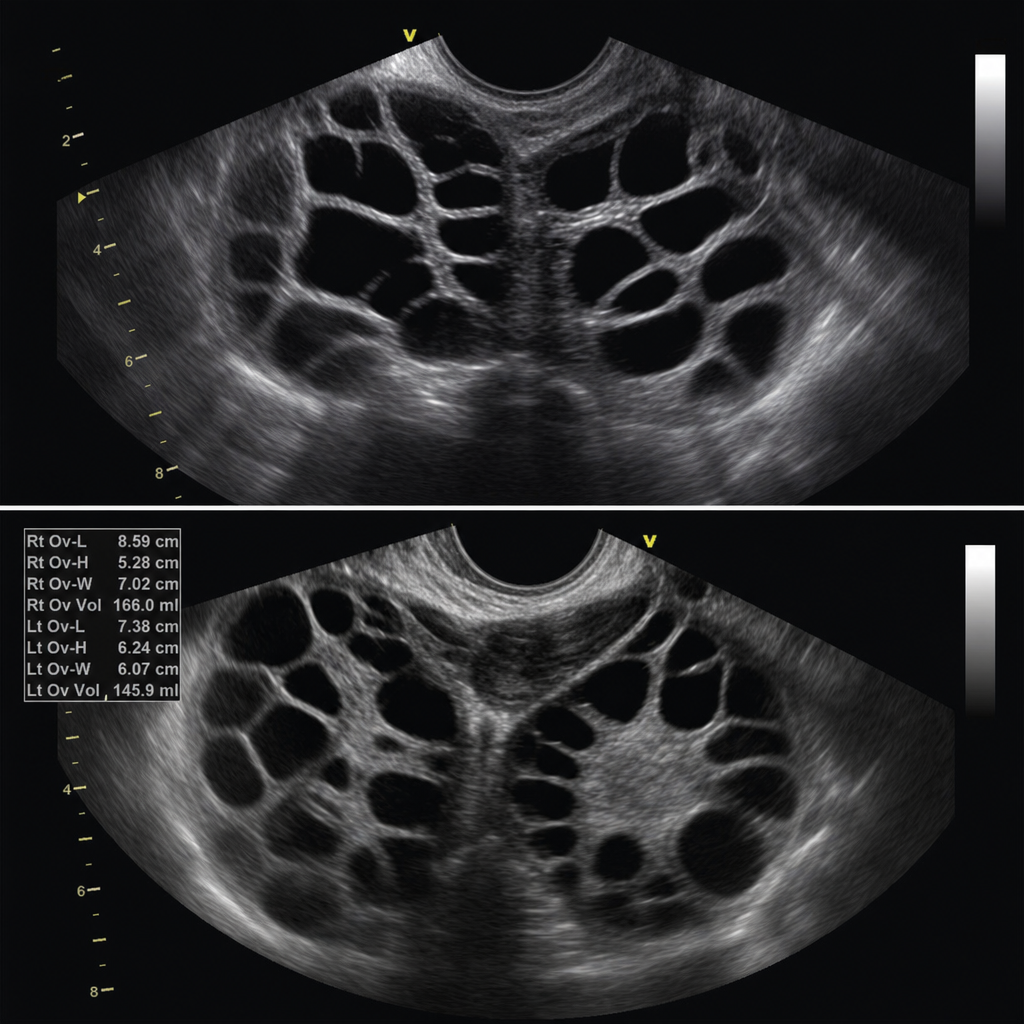
A female undergoing treatment for infertility with IVF was given Inj. HCG, presented with a history of vomiting, nausea, and headache. The USG is shown as below, what is the diagnosis?
Practice by Chapter
Reproductive Physiology
Practice Questions
Evaluation of the Infertile Couple
Practice Questions
Male Factor Infertility
Practice Questions
Female Factor Infertility
Practice Questions
Ovulatory Disorders
Practice Questions
Tubal and Peritoneal Factors
Practice Questions
Uterine Factors
Practice Questions
Unexplained Infertility
Practice Questions
Assisted Reproductive Technologies
Practice Questions
Psychological Aspects of Infertility
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app