
Fertility and Infertility — MCQs

On this page
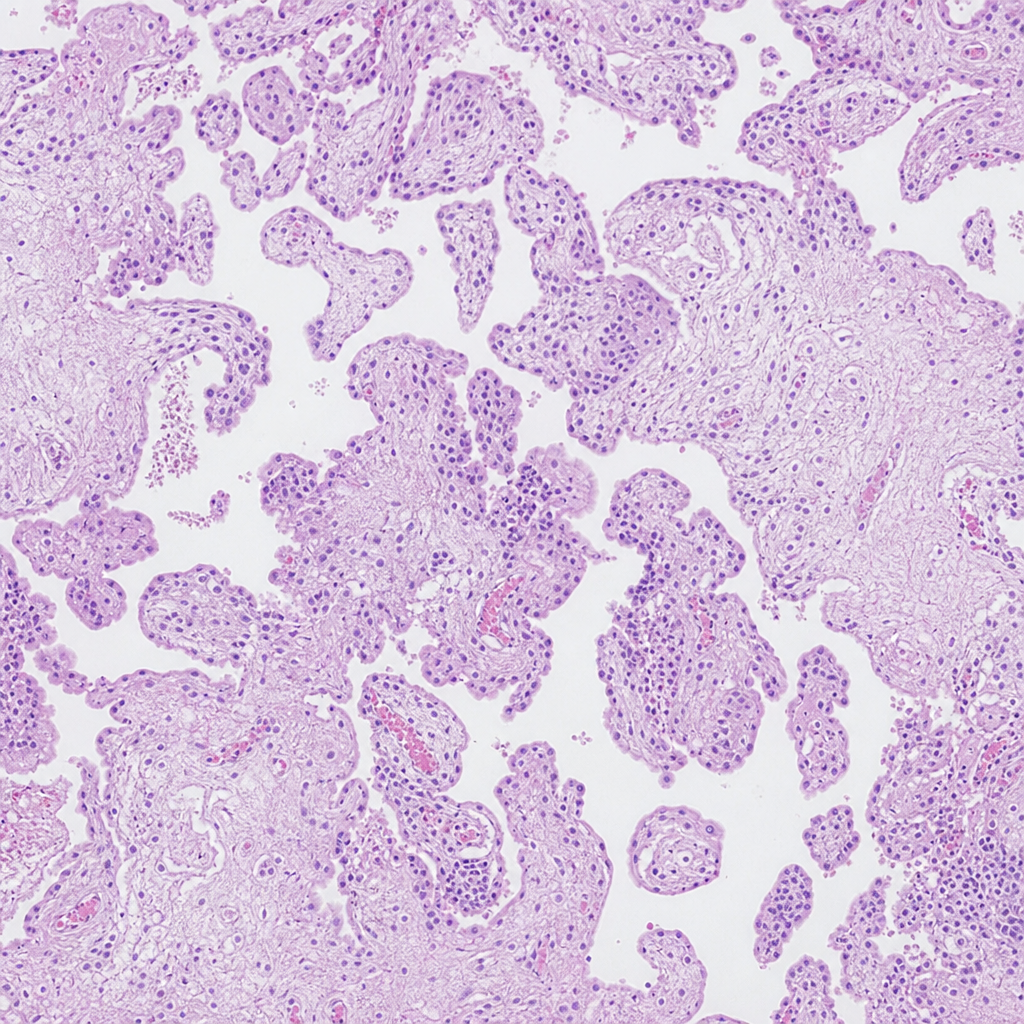
A 22-year-old woman presents at 14 weeks of gestation with excessive nausea, uterine size larger than dates, and a serum beta-hCG of 450,000 mIU/mL. Ultrasound shows a 'snowstorm' appearance. Suction evacuation is performed and the specimen is sent for histopathological examination. The histopathology is shown in Image 1. Which of the following best describes the karyotype and mechanism of origin of this condition?
A 27-year-old woman with Kallmann syndrome (congenital GnRH deficiency) desires pregnancy. She has been on estrogen-progesterone replacement for bone health. Her physician plans to switch her to pulsatile GnRH therapy. After 6 weeks of treatment, labs show: LH 4 mIU/mL, FSH 5 mIU/mL, estradiol 120 pg/mL. Ultrasound shows a 16mm dominant follicle. Evaluate and synthesize the physiologic response to determine the appropriate next intervention for ovulation induction.
A 28-year-old woman presents to the clinic for evaluation of infertility. Her menstrual cycles have been regular every 28 days. She reports using basal body temperature charting, which shows a biphasic pattern with temperature elevation occurring around day 14. Serum progesterone is measured on day 21 of her cycle and is found to be 18 ng/mL (normal luteal phase >10 ng/mL). Based on this information, what is the most likely status of her ovulatory function?
Clomiphene citrate challenge test (CCCT) is used for what purpose?
In Polycystic Ovary Disease (PCOD), which of the following drugs is NOT used for infertility management?
Practice by Chapter
Reproductive Physiology
Practice Questions
Evaluation of the Infertile Couple
Practice Questions
Male Factor Infertility
Practice Questions
Female Factor Infertility
Practice Questions
Ovulatory Disorders
Practice Questions
Tubal and Peritoneal Factors
Practice Questions
Uterine Factors
Practice Questions
Unexplained Infertility
Practice Questions
Assisted Reproductive Technologies
Practice Questions
Psychological Aspects of Infertility
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app